BACKGROUND
The loss of an unborn child, whether through miscarriage, stillbirth, or other complications, is a profound and intricate traumatic experience that can have psychological implications for women (Blackmore et al., 2011). Reactions after this loss generally include sadness, despair, guilt, anger, profound emptiness, and a persistent sense of loss (Kersting & Wagner, 2012; Slot et al., 2022; Voss et al., 2020). While parents may not have had the opportunity to fully engage with their infant, many still form a significant emotional bond with their unborn child during pregnancy, which can profoundly shape their grief response following a loss. Consequently, the intensity of grief and distress following pregnancy loss is often comparable to that experienced in other types of loss. For example, in a longitudinal investigation by Engelhard et al. (2001), 25% of women met the diagnostic criteria for acute stress disorder (ASD) within one month following a miscarriage. Similar patterns emerge in the case of stillbirth, where individuals reported experiencing moderate to high levels of ASD shortly after the loss (Murphy et al., 2014). According to these findings, contemporary models of perinatal grief (e.g., Wright, 2016) propose that parents frequently undergo intense grief and distress in the short term, gradually come to terms with their loss over time, and adapt to living in the aftermath of this life-altering experience. The most profound grief reactions typically diminish within the initial 12 months and significantly lessen after approximately two years (Badenhorst & Hughes, 2007; Brier, 2008). Nevertheless, in some individuals, the emotional impact of pregnancy loss can extend beyond the immediate grieving period, influencing various dimensions of a woman’s physical and mental health (Quenby et al., 2021).
Pregnancy losses typically occur suddenly and unexpectedly, leaving women little time to anticipate grief or prepare for the profound change in their circumstances. In some cases, however, a woman may have some expectation of loss (e.g., if fetal abnormalities are detected, or in instances where she chooses to terminate the pregnancy), though this awareness does not necessarily reduce the emotional impact (Gold et al., 2016; Goldstein et al., 2018). While grief is a natural and non-pathological process, the lack of preparedness and the traumatic nature of pregnancy loss can give rise to complicated grief, characterized by more disruptive, enduring, or pervasive symptoms than a typical grief response (Beutel et al., 1996; Kersting & Wagner, 2012; Shear, 2015). One of the characteristic symptoms of complicated grief in women with pregnancy loss is persistent self-blame, which potentially prolongs the regular grieving process, mainly when there are mixed emotions regarding the pregnancy or if individuals perceive having made a transgression (e.g., smoking or engaging in strenuous activities during pregnancy) (Friedman & Gath, 1989; Omar et al., 2019). Another distinctive aspect of complicated grief involves women continuously feeling a sense of bodily failure and a perceived undermining of their femininity (Frost & Condon, 1996; Riggs et al., 2020). Moreover, individuals may experience long-term jealousy toward others with children (Fernández-Basanta et al., 2022; Kersting & Wagner, 2012). These women often find it difficult to engage with friends or family members who have children or are at the same pregnancy stage at which their loss occurred (child envy). Overall, a high level of complicated grief is related to poorer mental health. For instance, Kersting et al. (2007) showed that the complicated grief that often accompanies pregnancy loss can lead to symptoms of depression, anxiety, and post-traumatic stress disorder (PTSD), which in turn significantly decrease women’s overall satisfaction with subsequent life. Due to the potential negative consequences of losing a child, further research should concentrate on psychological mechanisms that can provide appropriate support and interventions to help women navigate this challenging journey and break or reduce the negative impact of complicated grief on quality of life.
Lazarus and Folkman’s (1984)stress and coping theory offers a comprehensive framework for comprehending the experiences and coping strategies of women who have endured pregnancy loss. This model revolves around the cognitive appraisals made by individuals to evaluate and respond to stressors, emphasising stress as a dynamic process arising from the interaction between an individual and their environment. In the context of pregnancy loss, women confront a profound life stressor that can trigger diverse psychological reactions. In this paradigm, the development of complicated grief is likely to occur when women perceive the loss of their child as a substantial threat, harm, or challenge to their emotional well-being and life plans, which in turn initiates the process of actively coping with stressors. Conversely, secondary appraisals and coping, involving effective resource utilisation, may curb symptoms of complicated grief and substantially impact women’s mental well-being, adjustment, and overall quality of life (Murray & Terry, 1999; Swanson, 2000).
Sociodemographic and contextual variables have demonstrated limited utility in forecasting the intensity of responses to pregnancy loss (Horesh et al., 2018; McSpedden et al., 2017). The absence of compelling evidence connecting these factors to responses following infant death/abortion of the embryo leads researchers to explore alternative moderators of parental reactions to such tragic events. According to Lazarus and Folkman’s (1984) model of stress and coping, an individual’s adaptation to stress is mainly influenced by the availability of personal and environmental resources. Similarly, Skalski et al.’s (2022) model of coping with pandemic grief in COVID-19 suggests that perceived social support and personal resilience affect healing and significantly reduce the level of acute mourning and complicated grief. The authors propose that for achieving optimal adjustment to traumatic events and preserving mental well-being, it is crucial for both the mentioned mental resources (comprising environmental and personality variables) to coincide and work in conjunction. It is therefore probable that social support and resilience can break the negative impact of prolonged grief on the quality of life of women who experienced pregnancy loss.
Social support can play a pivotal role in the recovery process for women following pregnancy loss. This resource, characterised by empathy and understanding from family and friends, provides a vital channel for women to express their emotions and mitigates feelings of isolation that often accompany complicated grief (Abboud & Liamputtong, 2005). Social support, as defined by Cobb (1976), encompasses the advantages associated with feeling loved and valued, as well as being part of a “network of communication and mutual obligation” (p. 300). Social support provides relief and fosters a sense of belonging and connectedness. By offering connection, it aids in the grief process and contributes to women’s overall well-being and adaptation (Randolph et al., 2015). According to the buffering hypothesis, having solid social support benefits individuals dealing with stress. However, when no significant stress is present, it neither provides benefits nor causes harm (Fleming et al., 1982). To put it differently, low levels of support do not inherently induce stress and only put individuals at a comparative disadvantage when faced with exceptional stressors. Numerous research studies have demonstrated interactions between stress and support, suggesting that social support is particularly beneficial when confronted with high stress or grief levels (Song et al., 2023; Wang et al., 2021).
Resilience, described as the ability to adapt and bounce back from adversity (Konaszewski et al., 2021), may be a critical resource alongside social support in adaptation to adversities (Yıldırım & Solmaz, 2022) and be viewed as a buffer with a healthy outcome following exposure to risk (Hjemdal et al., 2006). While social support provides a crucial external resource, resilience represents an internal psychological strength that leads to better psychological adjustment, lower levels of depression and anxiety, and an enhanced overall sense of well-being (Schwartz et al., 2018; Skalski et al., 2022; Vegsund et al., 2019; Zhai & Du, 2020). Resilient people often demonstrate a greater capacity to cope with grief, accepting the loss and finding meaning in it (Friborg et al., 2003). Resilience enables them to rebuild their lives and relationships, fostering a sense of hope and optimism for the future (Rutter, 2012). Vegsund et al. (2019), in a Norwegian cross-sectional national survey conducted among bereaved parents, found that resilience is essential to predict healthy outcomes in people exposed to adverse life events. Nevertheless, research on resilience during grief over pregnancy loss is scarce, and available studies have not evaluated resilience as a protective factor that mitigates the adverse mental health effects of complicated grief, contributing positively to the quality of life for women following pregnancy loss.
Since individuals often seek solace and support in their faith and transcendence connections during times of crisis, it seems interesting to include spirituality in the corpus of research on coping with complicated grief after pregnancy loss. Spirituality is an individual’s search for and connection with the divine (Hill & Pargament, 2003; Park, 2007). In a broader context, it represents a feeling of existential contentment marked by a belief in the significance of one’s existence (Surzykiewicz et al., 2022). Spirituality is a coping method when individuals face diverse traumatic and challenging situations (Arévalo et al., 2008; Bryant-Davis & Wong, 2013; Davis et al., 2008; Gall, 2006; Maier et al., 2022). A higher level of spirituality is associated with positive outcomes, including better mental health (Garssen et al., 2020) and greater optimism, self-esteem, and life satisfaction (Aglozo et al., 2021; Fastame et al., 2021). Great suffering following the loss of a loved one profoundly affects the spiritual dimension, as individuals strive to find meaning and healing amid their pain (Wright, 2017). Extensive research demonstrates that spirituality is a resource frequently drawn upon by individuals during grief (Becker et al., 2007; Wortmann & Park, 2008; Zakar et al., 2018). A recent meta-synthesis of 21 studies in parents following stillbirth emphasised that the spiritual resources employed by mothers in their grieving process play a pivotal role in helping them discover meaning, maintain hope, and muster inner strength (Alvarenga et al., 2021). These resources encompassed an ongoing connection to their deceased baby, meaningful beliefs and rituals, and connections to themselves, the divine, others, and nature. Although a significant amount of literature suggests that spirituality may be protective in the case of adversities, its function in coping with complicated grief is not entirely understood yet. On the other hand, the moderating role of spirituality surfaced in the negative relationship between overall stress and health (the relationship was statistically significant only if spirituality was low) (Fenzel & Richardson, 2022; Kumar & Kumar, 2014). Similarly, in the study of Eames and O’Connor (2022), spirituality moderated the relationship between post-traumatic growth and deliberate rumination (the positive relationship was significant when spirituality was high). Furthermore, Ahmad et al. (2023) found that spiritual bypassing – the use of spiritual beliefs to avoid facing unresolved emotional issues – played a moderating role in the relationships between religious coping and psychological distress. Specifically, positive coping was significantly associated with lower levels of depression and anxiety, but only when there was a low level of spiritual bypassing. Available outcomes suggest that spirituality can help women maintain their overall well-being despite the emotional challenges of pregnancy loss. More precisely, spirituality could be meaning-making, allowing women to reframe and navigate the profound grief more effectively, by which the intensity of pregnancy grief would not necessarily translate into a lower quality of life.
The purpose of this study is to increase knowledge about positive adjustment to pregnancy loss. The literature review suggests that social support, resilience, and spirituality can buffer the negative impact of complicated grief on mental health. Therefore, we test the hypothesis that these resources will mitigate negative associations between complicated grief in women with pregnancy loss and quality of life, such that the relationship between complicated grief and quality of life will only be significant when the levels of social support, resilience, and spirituality are low.
PARTICIPANTS AND PROCEDURE
PARTICIPANTS
This study was conducted between 2018 and 2020 following approval of the study by the university’s ethics committee. For analyses, we included data from a sample of 333 women with a pregnancy loss history, aged 18-67 years (M = 34.58, SD = 7.66). Recruitment was in medical centres in Bavaria (Germany) and thematic support groups organised by Caritas Germany (the leading social service provider for people in mental health crises in Bavaria). The conditions for participation were female sex, legal age, and pregnancy loss. Meeting additional conditions was not required. Among participants, the time that had passed since the pregnancy loss was from a few months to 44 years (M = 5.25, SD = 6.42). On average, women had lost their pregnancy in the 20th week of pregnancy (SD = 11.14; min = 5, max = 42). Pregnancy loss was mainly spontaneous (85%). The cause of the pregnancy loss was known by 41% of participants. Among participants, 34% did not have living children, 32% had one child, 20% had two children, 9% had three children, and those remaining had more than three children. Most participants (64%) were employed during pregnancy. Of the participants, 30% lived in rural areas, 26% in small cities (less than 25,000 population), 22% in medium-sized cities (between 25,000 to 100,000 population), and 22% in major cities (more than 25,000 population). As regards education, 10% of participants had graduated from primary school, 41% from secondary school, and 49% from post-secondary education. Regarding marital status, most participants were in a stable relationship (77%). Catholics (35%) and Protestants (31%) predominated; only 30% of women declared a lack of religious affiliation. The study procedure involved completing paper-pencil questionnaires assessing grief after pregnancy loss, spirituality, social support, resilience, and quality of life, which took approximately 15 minutes to answer.
MEASURES
The Munich Grief Scale (MGS) was adapted from the Perinatal Grief Scale to assess complicated grief responses stemming from perinatal loss (Beutel et al., 1996). The MGS comprises 22 items categorised into five factors: sadness, guilt, anger, search for meaning, and fear of future loss, with responses rated on a five-point Likert scale from 0 (not at all) to 4 (completely). Higher scores on the scale indicate a more profound level of complicated grief. The scale exhibited satisfactory reliability and validity, as evidenced by its associations with measures of depression, anxiety, and physical symptoms (Beutel et al., 1995). Our study used an overall score with a Cronbach’s α of .92 (a single factor explained 41% of the variance). Sample items include: “I miss the baby,” “I blame myself for the death of the baby.”
Spirituality Scale. To measure spirituality, we developed the 14-item Spirituality Scale (see Appendix 1), which defines spirituality as the focused pursuit of the sacred, representing the central aspect of religion in an individual’s life (Pargament, 1997). A high score on the scale indicates a connection with the Creator and trust in Him. Participants ranked each statement on a five-point Likert scale from 0 (not at all) to 4 (completely). We decided to develop a new scale to embed the measurement of spirituality in the specific context of loss and grief. To assess the validity of the new questionnaire, we asked participants the question, “Overall, how would you rate your spirituality on a scale of 1 (not at all) to 6 (high)?” The correlation between the response to this question and the score of the developed scale was r = .62 (p < .001), indicating satisfactory convergent validity. To assess the structure of the scale, we randomly divided the participants into two groups. In the first group (N = 167), we performed exploratory factor analysis (EFA), which revealed a single-factor scale with standardized loadings ranging from .54 to .88 (α = .94), and this factor accounted for 59% of the variance. In the second group (N = 166), we performed confirmatory factor analysis (CFA), and its results confirmed the single-factor nature of the scale, χ2(77) = 75.22, p = .536; χ2/df = 0.98; RMSEA = .065, 90% CI [.059; .069]; SRMR = .04. Standardized loadings in the second group ranged from .45 to .82 and coefficient α was .91.
The Perceived Social Support Scale. We developed the Perceived Social Support Scale to assess social support. This 16-item scale (see Appendix 2) refers to emotional support, practical support, social companionship, and spiritual support. Participants ranked each statement on a seven-point Likert scale from 1 (disagree completely) to 7 (agree completely). A high score on the scale indicates a high level of perceived social support. We opted to create a novel scale to incorporate the assessment of social support within the specific context of pregnancy grief. To gauge the validity of the new questionnaire, we asked participants to indicate the number of people from whom they received social support after a pregnancy loss. The correlation between the number of social support providers and the scores from the developed scale was r = .47 (p < .001), indicating an acceptable level of convergent validity. We randomly divided the participants into two groups to examine the scale’s structure. Using data from the first group (N = 167), we conducted EFA, revealing a single-factor scale (standardized loadings ranged from .51 to .85) with high internal consistency (α = .93). This single factor accounted for 55% of the variance. In the second group (N = 166), we carried out CFA, which confirmed the one-factor structure of the scale, as indicated by the following fit indexes: χ2(104) = 113.12, p = .254; χ2/df = 1.08; RMSEA = .071, 90% CI [.051; .081]; SRMR = .05. Standardized loadings in the second group ranged from .47 to .88 and coefficient α was .92.
The Resilience Scale (RS-11), validated by Schumacher et al. (2005) and Kocalevent et al. (2015), was used to assess an individual’s level of resilience, which is regarded as a positive personality trait contributing to enhanced personal adaptation, linked to healthy development and the ability to withstand psychosocial stressors (Wagnild & Collins, 2009). Respondents rate their agreement on a seven-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree). The RS-11, designed as a unidimensional scale, has demonstrated its reliability and validity as a cost-effective tool for assessing resilience in the general population (von Eisenhart Rothe et al., 2013). In this study, the Cronbach’s α coefficient for the RS-11 was .82. Sample items include: “I have enough energy to do everything that I must,” “When I have plans, I follow them through.”
The WHOQOL-BREF. To assess quality of life in physical and psychological health, social relations, and environment, we used nine items from the WHOQOLBREF (The WHOQOL Group, 1998). All statements were rated on a five-point scale from 0 (not at all) to 4 (completely), with higher scores reflecting higher quality of life. The WHOQOL has displayed good divergent validity, content validity, and test–retest reliability (Skevington et al., 2004). The nine items were arranged into a single factor (α = .88) that explains 51% of the variance. Sample items include: To what extent are you satisfied with… “your health?” and “your ability to handle everyday tasks?”
STATISTICAL DATA ANALYSES
We conducted statistical analyses using R (R Core Team, 2023). All the variables of interest exhibited a normal distribution, as indicated by skewness (< |2.0|) and kurtosis (< |3.0|) values within acceptable limits. Prior to analysis, standardisation of all variables took place. The presence of multicollinearity was ruled out by assessing variance inflation factors. Descriptive statistics are presented in the form of means with standard deviations. To examine relationships among relevant variables, we conducted correlation analyses. Our research employed bias-corrected bootstrapping techniques to assess the moderation effect. A parameter was considered significant if the 95% bias-corrected confidence interval (CI) did not encompass zero after 5,000 bootstrapped samples.
RESULTS
PRELIMINARY ANALYSIS
In the first step of the analysis, a common bias testing method was employed. Based on Harman’s single-factor test, 50 principal components without rotation were extracted. The result showed that the first component explained only 33.1% of the total variance, below the critical threshold of 40% (Zhou & Long, 2004). Consequently, there was no significant common bias in the data.
BIVARIATE CORRELATIONS OF MAIN STUDY VARIABLES
Table 1 displays the means, standard deviations, and correlations between the variables involved in hypothesis testing. The correlation matrix showed that complicated grief after pregnancy loss was significantly negatively correlated with spirituality, resilience, and quality of life. Spirituality was positively associated with social support, resilience, and quality of life. Social support was positively linked to resilience and quality of life. In contrast, resilience was positively correlated with quality of life.
DEMOGRAPHIC CORRELATES
Time that had passed since the pregnancy loss was positively linked with social support (r = .15, p = .006), resilience (r = .11, p = .042), and quality of life (r = .17, p = .002). The reason for the pregnancy loss (0 – spontaneous, 1 – induced/planned) was negatively correlated with spirituality (r = –.13, p = .023). Furthermore, marital status (0 – single, 1 – partnered) was positively associated with spirituality (r = .20, p < .001), resilience (r = .21, p < .001), social support (r = .16, p = .003), and quality of life (r = .26, p < .001), and negatively associated with complicated grief (r = –.14, p = .009). Other sociodemographic variables were not significantly associated with the main study variables.
Table 1
Means, standard deviations, and Pearson correlations (N = 333)
Table 2
Moderating effects of spirituality in the relationship between complicated grief after pregnancy loss and quality of life (N = 333)
HYPOTHESIZED RELATIONSHIPS
Control variables that were included in all models as predictors of quality of life were age, the time that has passed since the pregnancy loss, the reason for the pregnancy loss, the number of living children, employment status, domicile, education level, marital status, and religious affiliation. Main effects of control variables and grief, spirituality, social support, and resilience are provided in Step 1. Interaction tests are shown in Step 2. Of particular importance, the results indicated a significant negative relationship between complicated grief after pregnancy loss and quality of life levels. At the same time, spirituality and the interaction between complicated grief after pregnancy loss and spirituality were found to significantly predict the quality of life. Notably, the negative correlation between complicated grief and quality of life was significant only in women with a lower level of spirituality (B = –0.13, t = –4.89, p < .001, 95% CI [–.181; –.078]), while in those with a higher level of spirituality, the relationship between independent and dependent variables was insignificant (B = –0.02, t = –1.44, p = .151, 95% CI [–.044; .007]) (see Table 2). Regarding social support, we observed a significant positive direct effect and an interaction effect with complicated grief on quality of life. Similar to spirituality, the relationship between complicated grief and quality of life was statistically significant only among women with lower levels of social support (B = –0.05, t = –2.84, p < .001, 95% CI [–.082; –.015]). For those with higher levels of social support, there was no significant link between complicated grief and quality of life (B = –0.003, t = –0.18, p = .854, 95% CI [–.036; .030]) (see Table 3). For resilience, the findings pointed to its positive direct relationship with quality of life. Nevertheless, the interaction effect of complicated grief with resilience was nonsignificant in predicting quality of life (see Table 4).
Table 3
Moderating effects of social support in the relationship between complicated grief after pregnancy loss and quality of life (N = 333)
Table 4
Moderating effects of resilience in the relationship between complicated grief after pregnancy loss and quality of life (N = 333)
Figure 1
Interaction between complicated grief and spirituality, social support, and resilience in relation to quality of life in women with pregnancy loss (N = 333)
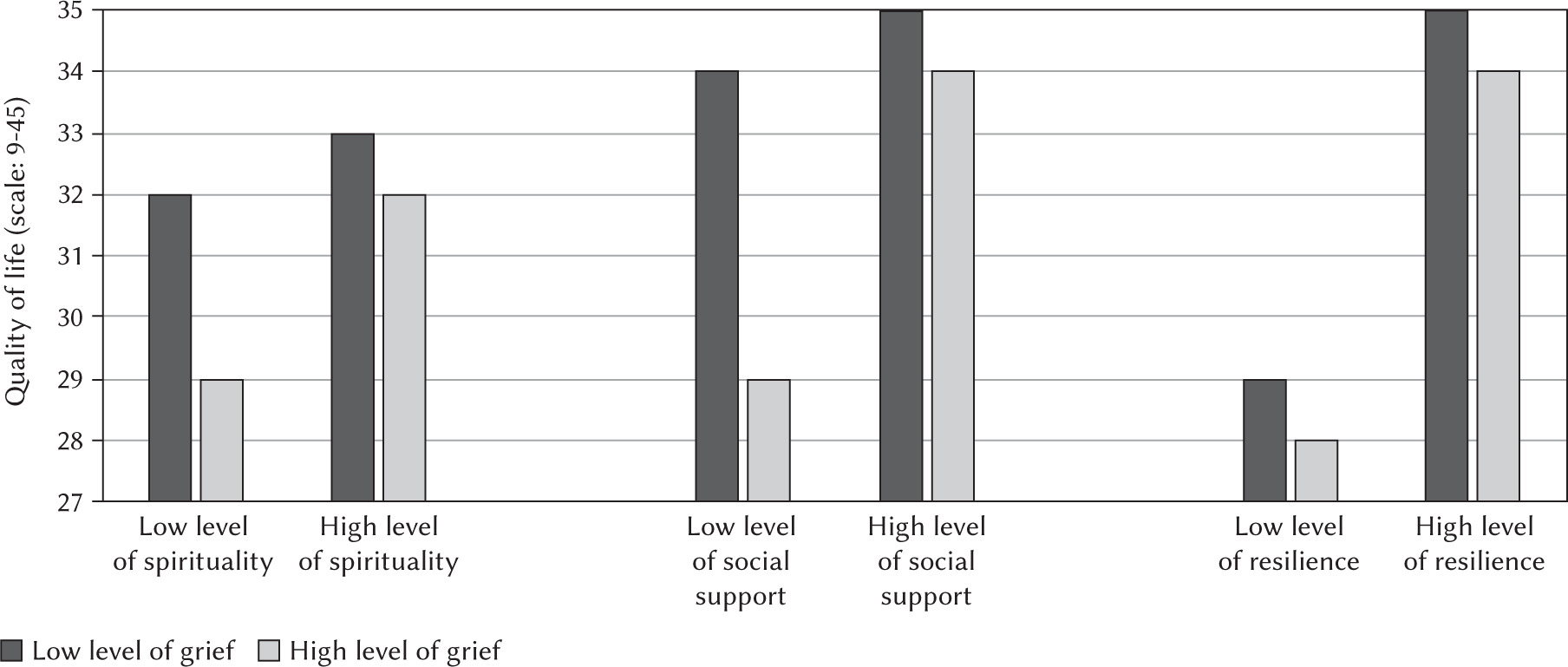
Figure 1 contains the results of simple effects analyses. The analysis of simple effects revealed that in the case of high levels of pregnancy grief, females with low levels of spirituality (M = 28.9, SE = 0.80) reported a significantly lower quality of life than women with high levels of spirituality (M = 32.1, SE = 0.86). Similarly, in women with high levels of pregnancy grief and low social support (M = 29.0, SE = 1.04), the quality of life was significantly lower compared to females with high levels of pregnancy grief and high social support (M = 33.9, SE = 1.14). Other comparisons proved to be statistically nonsignificant.
DISCUSSION
The present study aimed to deepen our understanding of the moderators of the relationship between complicated grief after pregnancy loss and quality of life in women. To our knowledge, we may be among the first to show that spirituality can mitigate this negative association. More specifically, the relationship between grief and life quality only existed when loss survivors presented a low level of spirituality. To some extent, this finding aligns with previous research highlighting the nature of spirituality as a coping mechanism during grief (Becker et al., 2007; Wortmann & Park, 2008; Zakar et al., 2018) and with modern spiritual and religious thought that often emphasizes seeking solace and hope during challenging circumstances (Kornfeld, 2009; Rohr, 2019). Fabricatore et al. (2000) and Fenzel and Richardson (2022) found a similar buffering effect concerning the relationship of overall stressors with depressive symptoms, such that the link was weaker for those with higher levels of spirituality than those with lower spirituality. Therefore, it is likely that spirituality can provide a framework that often provides solace, meaning-making, and a sense of transcendence in times of emotional burden, which in turn may maintain a relatively satisfactory level of mental well-being. However, it should be noted that some researchers suggest a more nuanced perspective on the impact of spirituality on grief, acknowledging its dual role. Apart from its potential for positive coping, they also highlight the dark side of this phenomenon and the risk of encountering a spiritual crisis after loss characterised by profound existential questioning or a sense of life’s meaninglessness (Agrimson & Taft, 2009). Within this context, spiritual distress may hinder the resolution of grief by impeding one’s ability to derive meaning from the experience of loss (Alvarenga et al., 2021).
In addition to spirituality, our outcomes point to social support as a significant moderator of connections between complicated grief and quality of life in women with pregnancy loss. More specifically, females with limited social support showed adverse consequences of complicated grief for quality of life, while in those with stronger support, significant associations between these variables were not observed, aligning with the consensus in the literature indicating the crucial role of social support in recovery after loss (Randolph et al., 2015; Song et al., 2023; Wang et al., 2021). Our findings also agree with Chen’s (2022) study on more than 4,000 bereaved single older adult Americans, which showed that grief reactions are related to depression, and this relationship was strong when existing social support was low. In addition, Barth et al. (2010) and Lee et al. (2014) postulated that a robust social support network facilitates the development of an individual’s self-esteem and self-efficacy, making it easier to ward off the emergence of detrimental emotions and moods. Our study widens these findings and indicates that when a woman faces self-blame for pregnancy loss, social support helps her to cope with missing the baby by bolstering her perceived ability to experience emptiness, reducing both the extent and onset of inferiority.
The significant interaction effects support the stress-and-coping model (Lazarus & Folkman, 1984), which assumes that adaptive strategies can reduce the perceived burden and help in adjustment to challenging circumstances. Nevertheless, despite obtaining moderating effects, we still observed significant main effects of spirituality and social support. This may be explained by the hypothesis of ‘artifacts of a significant monotone negative interaction’ (see Cohen & Wills, 1985, p. 319). Because all female participants reported experiencing pregnancy loss within the past years, symptomatology level under low-grief or -stress conditions can hardly be assessed. This means it is impossible to establish a pure buffering effect in these variables’ influence on quality of life. Nevertheless, our report and others (e.g., Chen, 2022; Fabricatore et al., 2000; Fenzel & Richardson, 2022) confirm the assumption that with high levels of spirituality and social support, traumatic experiences such as grief do not necessarily lead to poor mental health outcomes.
Despite expectations, resilience was not a significant moderator in the relationship between complicated grief and quality of life. Several plausible explanations exist for this situation, but two seem especially interesting to highlight. First, the experience of intense stress associated with pregnancy loss can cause a drastic reduction in the availability of individual coping resources (Hobfoll, 2011). In such a situation, individuals might not have been able to use the full potential of resilience to break the negative impact of complicated bereavement on quality of life. Second, the concept of resilience, traditionally viewed as a positive psychological attribute associated with adaptive coping and recovery (Konaszewski et al., 2021; Vegsund et al., 2019; Yıldırım & Solmaz, 2022), may paradoxically threaten women who have experienced pregnancy loss. This opposite perception is because, for many people, bereavement is the state of their relationships with the deceased, and the unexpected resilience people display in the face of loss – where the anguish of grief diminishes more quickly and more fully than individuals’ predictions suggest – can imply a disconnect from departed loved ones (Moller, 2007). Thereby, women would recognise resilience in the wake of grief as squandering the opportunity to attain valuable self-knowledge based on the relationship with a lost child, inadvertently contributing to further distress in dealing with pregnancy loss. Nevertheless, a positive association between resilience and quality of life suggested that careful education on this internal psychological resource, which is focused on self-reconciliation and does not interfere with the perceived bereavement process but helps give meaning to feelings related to pregnancy loss, can increase mental health in women with complicated grief.
This study suggests that social support providers should tailor their interventions to encourage women to develop strong social support systems, offering emotional aid and tangible assistance during grieving. Future psychoeducation sessions could provide women with information on the importance of social support during the grieving process, elucidating its potential benefits. Such training could also involve skills education in effective communication, helping women articulate their needs to their support network (e.g., partners, friends, and family), and fostering a more responsive environment. Moreover, group therapies could create a safe space for women to share their experiences, thereby reducing isolation and reinforcing a sense of belonging within a supportive community. At the same time, healthcare providers can integrate spirituality into their support strategies, ensuring that they accommodate individuals’ spiritual needs. Intervention in this area may involve guiding mindfulness and meditation practices, encouraging women to connect with their inner selves and explore their spiritual dimensions. It could also include building group discussions or workshops that encourage participants to share their spiritual experiences and perspectives, fostering community. Furthermore, the therapy might encourage women to engage in spiritual practices or rituals that resonate with their beliefs, offering them a sense of purpose, meaning, and connection in the face of their loss. By integrating these elements, psychological intervention can empower women to cultivate and strengthen their social support and spirituality, potentially aiding in their healing and coping process following the profound experience of pregnancy loss.
Before drawing conclusions, the limitations of this study should be mentioned. Firstly, we employed a cross-sectional design; therefore, it cannot definitively ascertain whether spirituality or social support moderates the relationship between complicated grief and quality of life or if the direction of these associations is different. Secondly, we did not control the number of pregnancy losses in participants, though this factor can be correlated with the overall mental health of women. For instance, the study of Kuhl-mann et al. (2023) showed that the number of pregnancy losses was positively correlated with depression symptoms for females. Similarly, we did not control for other losses (during the data collection period, the COVID-19 pandemic occurred, which caused a wave of sudden deaths in Germany and around the world) and potential stressors in women that could be confounding variables in the analysis. Finally, most participants experienced spontaneous pregnancy loss. We recommend replicating this study in a group that includes more women undergoing abortion due to their own autonomous decisions. Although our study found no differences in grief patterns between these groups, the community of women who ended a pregnancy intentionally was underrepresented, making it still possible that planned pregnancy loss (as a deliberate decision) may differentially predispose women to complicated grief. In addition to addressing these limitations, future research could consider including perspectives of fathers. Fathers may present different patterns in coping with the trauma of losing their unborn baby. Additionally, a wider analysis should be undertaken in non-Judeo-Christian cultures, where other religious concepts may determine the dissimilar mechanisms underlying spirituality and its relationship with grief.
CONCLUSIONS
This study underscores the critical role of spirituality and social support as significant moderators in the complex interplay between complicated grief and the quality of life among women who have experienced pregnancy loss. Our findings highlight the importance of recognising and fostering spirituality and social support networks as components aimed at breaking the negative influence of complicated grief on the quality of life of these women. At the same time, our results suggest that resilience, while not a significant moderator, plays a relevant direct role in predicting the quality of life for these women, emphasising its value as a psychological resource for enhancing female overall well-being. Nevertheless, education in this regard should be prudent and precise. In a philosophical context, some women may begin to regret their resilience because of what resilience tells them about their significance vis-à-vis the loved baby they have lost. Further longitudinal and experimental studies are needed to delve deeper into the mechanisms underlying dealing with complicated grief and to inform the development of tailored interventions for women navigating the profound experience of child loss.