Background
There is increasing evidence that the social restrictions implemented by governments during the COVID-19 pandemic, such as school closures and stay-at-home orders, severely affected adolescents’ mental health (Samji et al., 2022). In addition to the direct disruption of their daily lives due to the necessity for social distancing, the consequences of the measures affected adolescents’ home environments, causing increased familial conflict and parental stress over employment or finances. Research shows that compared to before the pandemic, adolescents reported increased depression, anxiety, and loneliness, and overall deteriorated psychosocial wellbeing during the pandemic (Samji et al., 2022). However, there is also variability in the extent to which adolescents were negatively affected by the pandemic. Specifically, girls and adolescents with a lower socioeconomic position reported the most adverse outcomes (Reiss et al., 2024).
These patterns align with Life Course Theory (Elder, 1998), which posits that individual development and the resulting mental wellbeing are affected by the timing and context of sociohistorical events, and their intersection with social structures and stratification. Disruptions to personal, educational, and social domains, such as those brought about by the COVID-19 pandemic, can significantly challenge normative developmental trajectories. Importantly, this theory predicts that the influence of such events is not uniform, but that individuals at specific developmental stages may be disproportionately affected. For adolescents, the pandemic coincided with a critical period in development, disrupting the expected timing of key transitions, constraining personal agency, limiting access to age-appropriate social opportunities, and exacerbating patterns of pre-existing inequalities (Benner & Mistry, 2020). Indeed, adolescence is a vulnerable developmental stage characterized by rapid hormonal, bodily, and brain changes, during which a considerable proportion of youth struggle with mental wellbeing: About one in five adolescents suffer from a psychiatric disorder, which often persists into adulthood (Pfeifer & Allen, 2021). Particularly girls and adolescents with a low – subjective – socioeconomic position (SEP)1 are at risk for developing mental disorders (McLaughlin et al., 2012). In addition to the physical changes during adolescence, adolescents’ social world undergoes important changes. The influence of parents gradually decreases, and peers and friends (particularly in-school peers) take a more central role in adolescents’ lives, exerting increased influence on their behaviors and wellbeing (Rose & Rudolph, 2006). However, even though parents’ role in adolescents’ lives changes, parental support is still crucial during adolescence and plays a central role in the development of adolescents’ emotion regulation skills – which in turn are often implicated in the development of psychopathology. Here, gender differences are evident, and to some extent are influenced by gender role socialization processes (for an overview see Rose & Rudolph, 2006). Adolescent girls (more than boys) use social support to cope with stress, and their wellbeing is more closely tied to the (availability of) interactions with peers. Thus, the social support of friends and close family members directly and indirectly is likely to play a protective role in adolescents’ psychosocial wellbeing, especially for girls (Rose & Rudolph, 2006). Given the centrality of social contacts for their mental wellbeing, having to socially distance during the pandemic therefore might have negatively affected girls more than boys.
Given their vulnerability to the development of mental disorders during adolescence, it is important to understand which inherent psychological resources protect or enhance adolescent wellbeing, and as such can help them cope with adversities such as the challenges posed by the COVID-19 pandemic. The Reserve Capacity Model (Gallo et al., 2005) offers a framework for understanding mental health disparities and highlights how external and internal psychosocial assets (reserves) could mitigate the negative effects of a lower SEP on mental health. In this framework, social support can be seen as a positive external resource that fosters emotional regulation and adaptive coping. An internal psychological asset that has been shown to mediate between socioeconomic position and health (Schelleman-Offermans & Massar, 2020) is Psychological Capital (PsyCap; Luthans et al., 2017). PsyCap is a higher-order construct consisting of hope, efficacy, resilience, and optimism, and enhances one’s ability to navigate challenges. In a recent systematic scoping review that included 16 studies, Preston and colleagues (2023) found that PsyCap had a significant positive relationship with positive mental health outcomes in youth.
The current study
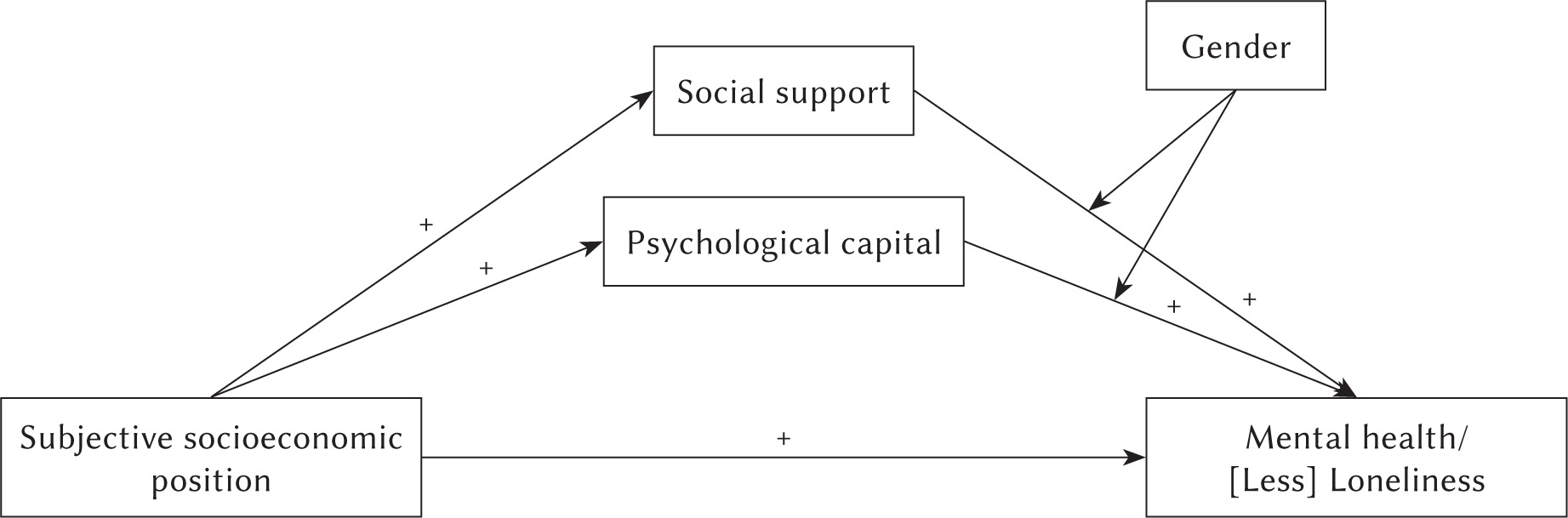
In the current research, we focused on perceived social support and PsyCap as possibly protective psychological resources that might help adolescents cope with the challenges of the pandemic and allow them to maintain psychosocial wellbeing. We explored whether (and how) these relationships differ as a function of adolescents’ subjective SEP. Furthermore, given the evidence that psychosocial wellbeing is lower among those with a lower SEP and among adolescent girls, we conducted two moderated mediation analyses to investigate gender differences in the mediating roles of PsyCap and social support (mediators) on the relationship between SEP (IV) and (a) mental health (DV), and (b) loneliness (DV). See Figure 1 for a visual representation of our expectations.
To this end, we utilized data that were collected between two periods of lockdown in the Netherlands (i.e., July–October 2021), at which point secondary school pupils were back to on-site education, yet other measures were still in place (e.g., keeping a 1.5-meter distance, work-from-home advice for adults, access to sports and cultural activities only with proof of vaccination).
Participants and procedure
Participants
Data collection took place at six secondary schools in the Limburg region of the Netherlands, between July and October 2021. Recruitment was aimed at pupils aged 13-16 years who were in year 2 or 3 of secondary school. In the Netherlands, secondary education is divided into three levels: pre-vocational education (VMBO, 4 years), senior general secondary education (HAVO, 5 years), and pre-university education (VWO, 6 years). Participants were recruited across all three educational levels. The sample (N = 498; 52.21% female, age M = 13.73, SD = 0.80) consisted of 31.6% pupils enrolled in the lowest level, 25.1% in the middle level, and 38.5% in the highest level. The data were collected as part of a cross-cultural collective project on adolescents’ psychosocial challenges during the pandemic (see Chung et al., 20242). Participating schools emailed an information letter with details on the aim and content of the study to parents. Parents who did not want their child to participate communicated this to their children’s teacher (i.e., opted out of consent). All participating pupils also provided individual informed consent. All materials and procedures for this study were approved by the local ethics committee (ref. ERCPN 188_10_2_2018_S94).
Procedure and measures
Data were collected during a regular (mentor) class, in which teachers provided the students with the link to the online Qualtrics questionnaire, gave some further information about the study, and were available to answer questions. Moreover, a research assistant who worked on the project and was familiar with the aims of the research and content of the survey was present to answer questions. Students completed the questionnaire on their mobile phone/tablet/laptop, which took 15-20 minutes. As an incentive and thank you for their voluntary participation, 20 online gift vouchers worth €25 were raffled among all participants. After reading an information page and providing their informed consent, pupils provided some socio-demographic variables (age, sex, educational year, and educational level). They then proceeded to complete the following measures (all translated into Dutch):
The MacArthur Scale of Subjective Social Status – Youth Version (Goodman et al., 2001) was used to measure socio-economic position (SEP). It depicts a ladder on which participants can indicate the subjective social standing of their family, relative to other families in society (scale 1 to 10).
The revised Mental Health Inventory-5 (MHI-5; Rivera-Riquelme et al., 2019) was used to assess the psychosocial well-being of adolescents during the COVID-19 pandemic, compared to before the pandemic. It consists of five items assessed with a 4-point scale from 1 (never) to 4 (always), so that a higher score indicates higher well-being (Cronbach’s α = .78). An example item is “Compared to before the pandemic, how often have you felt relaxed during the pandemic?”
Loneliness was measured using the UCLA 3-item Loneliness Scale (Hughes et al., 2004), asking participants how often during the pandemic they felt they lacked companionship, felt left out, and felt isolated from others (i.e., 1 – hardly ever; 2 – some of the time; 3 – often; Cronbach’s α = .78).
The Revised Compound Psychological Capital Scale-12 (CPC-12; Lorenz et al., 2016) was used to assess adolescents’ psychological capital. The self- report scale consists of 12 items measuring hope, optimism, resilience, and efficacy on a scale ranging from 1 (strongly disagree) to 6 (strongly agree). An example item is “I look forward to my life in the future.” Cronbach’s α = .90.
Social support was assessed with two questions: “Compared to before the corona crisis, how much more or less social support did you receive from [friends] [family]?” Answers were given on a scale from 1 (much less) to 5 (much more). These two questions were averaged (r = .22).
Results
Data were analyzed using SPSS v28 and the PROCESS macro (Hayes, 2017). First, descriptives and correlations were computed (see Table 1), revealing some gender differences. Follow-up independent sample t-tests showed that, compared to boys, girls reported lower mental health (girls M = 3.07, SD = 0.50; boys M = 3.31, SD = 0.48; t(472) = 5.33, p < .001), higher loneliness (girls M = 1.60, SD = 0.60; boys M = 1.47, SD = 0.52; t(465) = –2.49, p = .013), and lower PsyCap (girls M = 3.95, SD = 0.92; boys M = 4.18, SD = 0.94; t(441) = 2.61, p = .009). There was no significant gender difference in social support (girls M = 3.09, SD = 0.66; boys M = 3.14, SD = 0.68; t(464) = 0.79, ns).
Table 1
Correlations and means (SD) for the main variables included in the study
Next, we conducted two moderated mediation analyses, using the PROCESS macro (model 14; Hayes, 2017) to predict (1) mental health and (2) loneliness. We used SEP as the predictor, gender as the moderator, and PsyCap and social support as mediators. Given that some correlations between age, education, and our main variables exist, we included age and education level as covariates.
Mental health
For mental health, the full model was significant (F(8, 434) = 24.10, p < .001, R2 = .31). The direct effect of SEP on mental health was still present upon adding the moderated indirect effects, suggesting partial mediation (B = .059, t(434) = 3.89, p < .001), and indicating that individuals with a higher SEP reported better mental health. There was no moderation by gender for PsyCap (index of moderated mediation B = –.007, 95% CI [–.026, .010], SE = .009). This variable partially mediated the relationship between SEP and mental health in a similar manner for boys (B = .033, 95% CI [.015, .054], SE = .010) and girls (B = .025, 95% CI [.012, .042], SE = .008). For social support however, the index of moderated mediation was significant (B = .019, 95% CI [.002, .039], SE = .009). Specifically, social support only partially mediated the relationship between SEP and mental health for girls (B = .015, 95% CI [.004, .029], SE = .006), such that girls’ higher scores on social support were positively related to better mental health. For boys, social support did not act as a mediator (B = –.03, 95% CI [–.016, .007], SE = .006). Including gender as a moderator increased the variance explained in mental health from 24.9% to 30.8% (ΔR2 of 5.9%), representing a small effect size (f2 = 0.1).
Loneliness
For loneliness, similar results were found. The overall model was significant (F(8, 434) = 12.41, p < .001, R2 = .19). The direct effect of SEP on loneliness was still present, suggesting partial mediation (B = –.04, t(434) = –2.33, p = .020), and indicating that individuals with lower SEP reported higher loneliness scores. Again, no moderation of gender was present for PsyCap (index of moderated mediation: B = .006, 95% CI [–.010, .026], SE = .009), indicating that this variable partially mediated the relationship between SEP and loneliness in a similar manner for boys (B = –.028, 95% CI [–.049, –.013], SE = .009) and girls (B = –.022, 95% CI [–.039, –.009], SE = .008). Again, there was moderating effect of gender on social support (index of moderated mediation: B = –.020, 95% CI [–.42, –.002], SE = .010). Whereas social support did not act as a mediator for boys (B = –.001, 95% CI [–.017, .009], SE = .007), for girls the mediation was present (B = –.023, 95% CI [–.041, –.008], SE = .008). This result indicates that for girls, lower levels of social support caused them to report increased loneliness. Including gender as a moderator increased the variance explained in loneliness from 17.8% to 18.6% (ΔR2 of 0.8%), corresponding to a very small effect (negligible; f2 = 0.01).
Discussion
During the COVID-19 pandemic, the global prevalence of mental health problems among adolescents increased. To gain insight into how these youth may cope better during future pandemics, the aim of the current study was to investigate the mediating role of protective psychological (PsyCap) and psycho-social factors (perceived social support) in the relationship between subjective socioeconomic position and psychosocial wellbeing (mental health and loneliness) among Dutch adolescents. Given previous research findings about the positive influence of social support on students’ mental wellbeing during the pandemic (Magson et al., 2021), and the positive effect of PsyCap on mental health outcomes for youth (Preston et al., 2023), we chose these variables as mediators and included gender as a possible moderator.
Our results indicated that girls reported worse psychosocial wellbeing, i.e. lower mental health and increased loneliness, than boys. Moreover, for both boys and girls, having a lower SEP was associated with more loneliness and decreased mental health (see also Chung et al., 2024), whereas having a higher PsyCap and having more social support were associated with better mental health and lower loneliness scores (Preston et al., 2023). The moderated mediation analyses further indicated that boys and girls did not differ in the positive mediating role of PsyCap between SEP and either outcome variable. However, there was a gender difference for social support: it only acted as a mediator for girls, such that girls who reported increased social support also reported better mental health and lower loneliness. For boys, social support did not mediate the relationship between SEP and psychosocial wellbeing.
Overall, our findings align with Life Course Theory (Elder, 1998), which highlights the differential influence of cumulative (dis)advantage and social context across development in light of sociohistorical events. Moreover, the gendered effect of social support may reflect socialization processes that emphasize relational interdependence for girls, making supportive social ties particularly protective during adolescence. The findings also align with our previous research on the mediating role of PsyCap in explaining the SEP-health gradient (Schelleman-Offermans & Massar, 2020), and indicate that several psychological resources may protect young people against the adverse effects of having a lower SEP and/or contextual stressors like those they experienced during the pandemic. As such, our findings are in line with the reserve capacity model (Gallo et al., 2005), which also suggests that the adverse effects of having a lower SEP on physical and mental health might be reduced for individuals with greater amounts of intrapersonal (e.g., PsyCap) and interpersonal (e.g., social support) reserves. Given that PsyCap in particular is a construct that is sensitive to development, interventions aimed at increasing PsyCap may support young people in coping with adverse circumstances, for both boys and girls.
Our findings also suggest that social support is particularly important for girls in maintaining psychosocial wellbeing – this is in line with other research (Johansen et al., 2021) that shows that the protective role of social support for mental distress was mainly found among young women. Research (Magson et al., 2021) indicated that, during the pandemic, boys often coped through structured routines, physical activity, and online gaming, which offered distraction, autonomy, and social connection, thereby supporting their mental health. Thus, in times of stress, boys may benefit from structured, autonomy-supportive environments and possibilities for action-based coping like sports or games that also offer peer connections, whereas girls may prefer emotionally expressive support. However, given the mediating effect of PsyCap for both boys and girls, we suggest that adolescents may benefit from group-based activities that focus on enhancing resilience, hope, optimism, and efficacy, yet a different format may be preferred depending on gender.
Some limitations of the current research need to be acknowledged. First of all, some of the questions required pupils to reflect on their psychosocial wellbeing before the pandemic, which may have caused recall bias and under- or overestimation of symptoms (see Pacheco-Romero et al., 2025). Furthermore, we used a measure of subjective socioeconomic position, but we did not include family-level objective indicators for SEP, such as parental attained educational level, parental employment status, or income. However, there is increasing evidence that subjective well-being is more strongly associated with subjective SEP than with objective SEP (Tan et al., 2020). Lastly, since this was a cross-sectional study, causality cannot be established, and caution is required when interpreting our results.
To conclude, this study provides valuable insights into the factors that may protect adolescents from the adverse effects of low socioeconomic position and contextual stressors such as the COVID-19 pandemic. Our findings highlight the importance of both intrapersonal resources, such as PsyCap, and interpersonal resources, like social support, in promoting psychosocial well-being among young people. While PsyCap appears to be a protective factor for both boys and girls, social support seems to be particularly crucial for girls. These results emphasize the need for interventions that foster social connectedness, resilience, hope, optimism, and efficacy, particularly among girls, to help them cope with challenges and maintain their mental health. Future research should explore the long-term implications of these findings and investigate how interventions targeting these protective factors can be effectively implemented in educational and community settings.