Background
Post-traumatic stress disorder (PTSD) is a psychopathological response to a traumatic experience and related to trauma and stress. The experience can occur when someone faces a situation such as sexual assault, death, serious disease or war. PTSD can affect anyone after having experienced a traumatic event. PTSD is characterized by four symptom clusters: re-experiencing the event; avoiding things reminiscent of the trauma; negative physical and emotional reactions; and neurovegetative hyper-activation (American Psychiatric Association, 2013).
The most traumatic event experienced by adolescents may be the sudden and unexpected death of a loved one, with a percentage of 19.5% (Astitene & Barkat, 2022). In another study, it was 33.1% (Astitene et al., 2020).
There are very few studies on the prevalence of PTSD and its comorbid disorders among schoolchildren in Morocco. These studies show a high prevalence of PTSD in Morocco. Our study aimed to confirm or refute this high prevalence.
There is a lack of national data on the prevalence and correlates of PTSD among adolescents in Morocco. This research will help us understand the link between the Moroccan cultural context and this prevalence, especially in the context of poverty, precariousness, unemployment, and low parental education. Furthermore, this study examines whether this context can contribute to the development of PTSD by analyzing risk factors that may increase the likelihood of developing this disorder. The current study therefore investigated whether these factors influence the development of PTSD. This survey also aimed to study the relationship between PTSD in school-aged children and their academic performance.
If PTSD is left untreated, these symptoms worsen and persist for many years, which negatively influences the individual’s daily life. If these symptoms continue to persist more than a month after a traumatic event, they may be a sign of PTSD (American Psychiatric Association, 2000; Elia, 2023). Schoolchildren with PTSD may relive the trauma over and over again. They may have nightmares or flashbacks. They may also suffer from uncontrolled anxiety and unwanted thoughts. Therefore, they often avoid remembering the event.
The various symptoms observed in adolescents are almost identical to those in adults (Dyregrov & Yule, 2006). This disorder can cause negative effects such as sleeping problems, poor academic results, and frequent nightmares.
In Morocco, a study was conducted on 348 schoolchildren aged between 14 and 17 years (16.13 ± 0.81). The prevalence of PTSD was found to be 25.8% (Astitene & Barkat, 2022). Another study was conducted on 982 adolescents aged 12 to 17 years (14.98 ± 1.49). The prevalence of PTSD was estimated at 19.3% (Astitene & Barkat, 2021).
The factors found to predict PTSD were gender, repetitive dreams, interrupted sleep, memory difficulties, and difficulties in concentration (Astitene & Barkat, 2022).
The factors independently associated with PTSD included being a girl, interrupted sleep, guilt, difficulties with memory, and difficulties with concentration (Astitene & Barkat, 2021).
Adolescents who experience traumatic events may sometimes attribute responsibility to others for what occurred (Deering, 2000). Research has shown that parents may neglect the symptoms of their children’s stress (Stuber et al., 2005). It is strongly recommended that schoolchildren be interviewed directly to assess their PTSD symptoms (Kassam-Adams et al., 2006; Meiser-Stedman et al., 2007). In addition, adolescents voluntarily or involuntarily avoid telling their parents in detail about the impact of the traumatic event on them for different reasons and depending on the personality of each schoolchild (Vila & Bertrand, 2003).
The objective of this investigation was to determine the prevalence of post-traumatic stress disorder for schoolchildren in public schools in the city of Salé in Morocco. An additional aim was to study the effect of this disorder on their educational career and social life. In our investigation, the co-morbidities of PTSD that we were interested in were anxiety disorders and depressive disorders. These disorders have a direct negative effect on the school life of schoolchildren. We also assessed the effect of this disorder on the schoolchildren’s social and academic life, because PTSD can influence the adolescent’s daily life.
The investigation was conducted to help establish a support system for schoolchildren by Moroccan organizations to promote the quality of life at the psychological and academic levels. It is especially necessary due to the significant prevalence of post-traumatic stress disorder in Morocco. The main criteria that present risk factors for the development of PTSD are poverty, psychological states of adolescence, and the low level of education of parents. These factors reflect the specific situation of Moroccan schoolchildren. Moreover, this country is one of the low- and middle-income countries where there is a lack of medical intervention for schoolchildren who suffer from this disorder.
Hypotheses
Based on the study objectives, the following hypotheses were formulated:
H1. Age, gender, substance use, or exposure to a traumatic event could contribute to the development of PTSD.
H2. Comorbid disorders (anxiety and depression) are expected to be more prevalent in participants who suffered from PTSD.
H3. Quality of life may be disrupted in participants with PTSD: sleep disruptions, memory disruptions, difficulty concentrating, suicidal ideation, and disinterest in activities.
Participants and procedure
Population
The investigation was carried out in Salé city in Morocco. The survey was conducted in five municipal districts of Salé: Lamrissa, Tabriquet, Bettana, Laâyayda, and H’ssaine. For each district, we took 3 to 4 middle schools, depending on the number of schools in the district. There are 51 public middle schools, of which 18 were randomly selected for this study, representing 35.3% of the total. From each selected school, 50 students were sampled, resulting in a total sample of 900 schoolchildren. The cross-sectional survey was conducted between January and April 2020. Eligible participants included currently enrolled schoolchildren aged 11 to 16 years. Also, they were present during the study period and did not have a mental disability. Schoolchildren attended all three levels of school classes.
Informed consent forms were distributed to the parents or guardians of all 900 selected schoolchildren. Upon collection, 99 students did not return signed consent forms, resulting in a final sample of 801 participants. This corresponds to a participation rate of 89%. The age of these adolescents varied between 11 years and 16 years (M = 13.11, SD = 0.82). Schoolchildren attended all three levels of school classes, and some of them had to repeat their classes. Data are shown in the results section.
During the survey, 94 schoolchildren did not continue to fill out the questionnaires because they declared in the distributed questionnaire (CPTS-RI) that they had not experienced any traumatic event. This experience was defined as the most terrifying life event experienced, involving confrontation with death, fear of death, or serious injury, or when one’s physical integrity or that of another person has been threatened. Thus, after having declared having been exposed to at least one traumatic event during their life, 707 (88.3%) schoolchildren completed the investigation. These schoolchildren of both sexes were divided into 335 males (47.4%) and 372 females (52.6%). These events were mentioned in the life events checklist distributed to schoolchildren (the list had 17 events such as sexual assault, death, serious disease, war, accident, and heist).
We used the following inclusion criteria: (1) Have experienced or witnessed a potentially traumatic event, (2) currently in education, not exceeding the age of 17 years, (3) being present at the school during the investigation, (4) and having given informed consent.
The following exclusion criteria were applied: (1) Not currently in school, (2) exceeding the age of 17 years, (3) not having a mental disability, (4) and refusal to participate.
Cochran’s formula was used to calculate the sample size. The general formula is as follows:
n0 = Z2∙p∙(1 − p) / E2
n0 = initial sample size for large populations (before any adjustments for finite populations),
Z = z-value (e.g., 1.96 for 95% confidence),
p = estimated population proportion (0.5),
E = margin of error (5%).
Therefore, the theoretical sample would be: n0 = 1.962∙0.5∙(1 − 0.5) / 0.052 = 385
We increased the number to 900 individuals.
Regarding missing data, there were none, as all questionnaires were completed by the participants.
Procedure
We met individually with each school director to present the purpose of the study and explain all the steps to conduct this research at the school level. Also, it was necessary to agree on the choice of classes and students.
Another day, we met with the schoolchildren to listen to the questions relating to the investigation and then explain to them how the investigation would proceed. A third meeting was held, so that the parents or guardians of the schoolchildren clearly understood all the stages of the investigation. For each schoolchild, we gave a newsletter to give to their guardians. Also, to confirm the participation of these schoolchildren in this survey, these newsletters were provided with informed consents which must be signed by their guardians. At the next meeting with the schoolchildren, we welcomed those who agreed to carry out the survey with their signed informed consent. Immediately after, we distributed a sociodemographic questionnaire to be completed with social and demographic information. Then, another questionnaire presented a life events checklist to complete with data regarding the life events experienced by each schoolchild. For the last stage of the investigation, a final meeting was held for the distribution of three questionnaires: the Children’s Post-Traumatic Stress Reaction Index (CPTS-RI; Fernandez et al., 2005) for the collection of data concerning the state of stress post-traumatic; the State Trait Inventory Form Y (STAIY; Spielberger et al., 1983) to measure anxiety; and finally, the Children’s Depression Inventory (CDI; Fernandez et al., 2005) to measure depression. These questionnaires were distributed successively and were clearly explained. There were adolescents who did not continue to complete the questionnaires (CPTS-RI, STAIY and CDI) because they had not experienced any traumatic occurrence (Stuber et al., 2005; Vila & Bertrand, 2003). All questionnaires were completed anonymously and by the schoolchildren themselves.
Materials
We used five questionnaires to collect the data and distributed them successively as follows:
The sociodemographic data questionnaire.
The Life Events List; this list presents 17 questions regarding the most stressful events during an adolescent’s life, according to the DSM-5 (American Psychiatric Association, 2013).
The CPTS-RI questionnaire intended for children aged between 6 and 16 years. This questionnaire was carried out to define the symptoms of PTSD after exposure to a traumatic event, and the administration time was 15 to 20 minutes. This questionnaire presented a scale of 20 items, with each item of the scale divided into 5 levels. According to the calculation of the results of these levels, we obtain a score which determines the level of PTSD; a score lower than 12 means that the schoolchildren do not have PTSD. A score of 12 to 24 indicates a low level of PTSD, a score of 25 to 39 indicates a moderate level, a score of 40 to 59 indicates a severe level, and a score greater than 60 indicates a very severe level. Cronbach’s α for the CPTS-RI was high (.87), and the test-retest reliability was .67.
The STAIY is a self-assessment questionnaire; it is a scale which presents 20 items and which aims to measure the intensity of anxiety in schoolchildren. The duration was 10 to 15 minutes; each answer to a questionnaire item corresponds to a score from 1 to 4 (1 indicating the lowest degree of anxiety, 4 the highest degree). A score of less than 35 indicates a lack of anxiety, a score above 65 indicates very high anxiety, 56 to 65 indicates high anxiety, 46 to 55 indicates medium anxiety, and 36 to 45 indicates low anxiety. Cronbach’s α for the STAIY was .82, and the test-retest reliability at 8 weeks later was moderate (between .46 and .61 depending on the item studied).
The last self-assessment questionnaire to assess the level of depression was the CDI; it includes 27 items and aims to measure the intensity of depressive symptoms in adolescents. Each item is rated from 0 (absent or normal) to 2 (severe). The CDI targets children and adolescents aged 7 to 17 years. A score less than 15 indicates the absence of depression and a score equal to or greater than 15 indicates the presence of depression. The duration of handover is 15 to 20 minutes. Cronbach’s α for the CDI was .71, and the test-retest reliability at a one-month interval was .43.
Ethical approval
We obtained written approval for authorization of the research from the Ministry of National Education and Scientific Research. Informed consent forms signed by parents or guardians were obtained.
Statistical analysis
We used SPSS (version 20) to carry out all statistical analyses. Descriptive statistical analysis was used to present data as number (n) and percentage (%). Continuous variables were expressed as mean ± standard deviation. Comparisons of quantitative variables were performed using the Student’s t-test to determine whether there were significant differences between group means. When statistically significant differences were found, Cohen’s d was calculated to assess the effect size, indicating the magnitude of the difference between groups. The comparison of the qualitative variables was carried using the chi-square test (χ2), and Cramer’s V was used to measure the strength of association between nominal variables. We used Cramer’s V test, following a chi-square test, to measure the strength and intensity of the relationship between two qualitative (categorical) variables, because the chi-square test alone only indicates whether there is a significant association, but not its magnitude. A correlation (r) was established for a comparison between the continuous variables (frequency of tobacco use, level of PTSD, concentration level, level of anxiety, level of depression, memory difficulties, level of concentration, and suicidal ideation) using the Pearson correlation (to assess the strength and direction of a linear relationship between two quantitative variables, in order to determine whether a statistical association exists and to what extent the two phenomena vary together). A p-value of less than .05 was considered statistically significant for all analyses.
Results
Sociodemographic data and experienced traumatic events
All participating adolescents were aged 11 to 16 years (13.11 ± 0.82). 84.7% of participants had married parents, and 1.7% lived with their parents in slums. Among the schoolchildren surveyed, 3.6% had fathers who were unemployed, while 71.7% had mothers who were not working. The combined average monthly income of parents was 3.27 ± 1.61 thousand Moroccan dirhams (MAD; 1 MAD ≈ 0.10 USD or 0.09 EUR), suggesting that most families earned roughly between 1,660 and 4,880 MAD per month. Regarding substance use, 20.1% of schoolchildren reported tobacco use, and 10.2% reported using drugs. Additionally, 27.3% (n = 193) of the schoolchildren had repeated a grade.
This data indicate that the country where the survey was conducted is a low- to middle-income country.
According to the Life Events List completed by the schoolchildren, among 17 traumatic occurrences, 16 had been experienced. Participation in war was the only event that had not been experienced. 20.1% presented the percentage of the most experienced event, which was the abrupt and unexpected death of a loved one. It was followed by 11.2% for an event of intense human suffering. In Kenya, among adolescents, the percentage of abrupt and unexpected death of a loved one was 42% (Mbwayo et al., 2019), and in Morocco it was 27.7% (Astitene & Barkat, 2021).
This means that the abrupt and unexpected death of a loved one is a significant traumatic event linked to PTSD. For individuals who have experienced this, PTSD may develop if the normal grieving process is disrupted, leading to prolonged fear and distress instead of recovery, with symptoms such as flashbacks, nightmares, and intrusive thoughts. 4.43 ± 1.57 months was the average time since the traumatic event, which means that the traumatic event had occurred 3-6 months previously, as shown in Table 1.
Table 1
Variables expressed in number and percentage of students
Prevalence of post-traumatic stress disorder and associated disorders of PTSD
In our sample of 707 schoolchildren, we found that 31.7% (n = 224) had PTSD with a severe and very severe and moderate severity level. 68.3% (n = 483) of the schoolchildren did not have PTSD. Regarding gender among schoolchildren who had PTSD, we found 88 boys (39.3%) and 136 girls (60.7%).
Girls are at a higher risk for PTSD due to a combination of biological and psychosocial factors. Hormones such as progesterone can influence brain responses, potentially enhancing the recall of negative memories and making it harder to extinguish fear. Additionally, girls may be more likely to use a “tend-and-befriend” stress response, seeking social support or engaging in caregiving. While this strategy can be adaptive, it may also increase emotional vulnerability, contributing to a higher susceptibility to PTSD.
In Egypt, the prevalence of PTSD among adolescents was 16.3% (Rabie et al., 2015). In Kenya 26.8% of adolescents had PTSD (Mbwayo et al., 2019). In Tunisia, the prevalence was 37.4% among adolescents (Boudabous et al., 2023).
Hypothesis H1 was checked: girls had a higher risk of PTSD compared with boys.
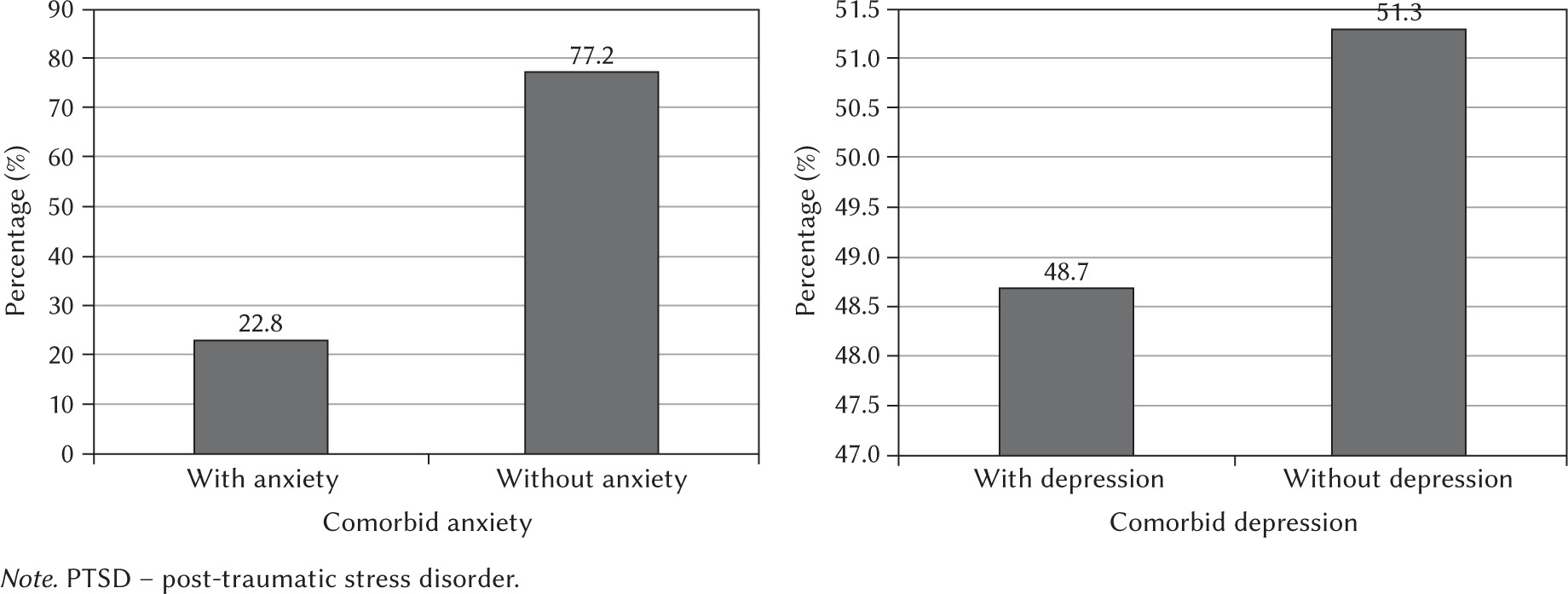
In the group with disorders associated with PTSD, we found that 77.2% had anxiety (n = 173) and 51.3% had depression (n = 115), as shown in Figure 1.
Regarding anxiety, 49.1% (n = 110) of affected schoolchildren were girls, compared with 28.1% (n = 63) boys. Similarly, for depression, 37.5% (n = 84) were girls, while 13.8% (n = 31) were boys. These findings indicate that female adolescents exhibited higher rates of both anxiety and depression, which are commonly comorbid with PTSD.
Hypothesis H2 was supported: the prevalence of anxiety and depression was higher in the group with PTSD than in the group without PTSD.
The high prevalence of anxiety and depression in individuals with PTSD means that these conditions are very common and often accompany the traumatic event that triggered the PTSD. The trauma itself, along with associated stressors (isolation, uncertainty, fear of death), causes significant psychological distress, which can lead to the development of anxiety and depression.
In Egypt, among adolescents, the percentage of depression was 33.3% (Mbwayo et al., 2019), and in Uganda it was 39% (Ainamani et al., 2022). In two studies in Morocco, among adolescents, the percentage of anxiety was 81% (Astitene et al., 2020) and 79.1% (Astitene & Barkat, 2021).
Factors associated with PTSD
We found that the group without PTSD was older than the group with PTSD (p = .031), and the effect size was medium (d = 0.43). Hypothesis H1 was supported: the group without PTSD was older than the group with PTSD.
The level of co-morbidities (anxiety and depression) was higher in the group with PTSD than in the group without PTSD (p < .001 and p < .001 respectively), with large and moderate effect sizes, respectively (d = 0.95 and d = 0.50). The participants with PTSD had more sleep disruptions than the group without PTSD (p = .027), with a large effect size (d = 1.12). Moreover, the PTSD group had memory impairments (p = .015) with a moderate effect size (d = 0.59), and difficulty concentrating (p = .018) with a large effect size (d = 1.13), as shown in Table 2.
Table 2
Difference in variables between adolescents without PTSD and adolescents with PTSD
Girls were younger than boys (p < .001) and the effect size was large (d = 0.69). Girls had a higher risk of PTSD compared with boys (p = .008) with a large effect size (d = 0.75). Girls with PTSD had a higher level of concentration difficulties than boys (p = .028) with a small effect size (d = 0.15). Girls with PTSD had more sleep difficulties than boys (p = .041) with a small effect size (d = 0.25). Boys had a higher frequency of smoking than girls (p = .023) with a moderate effect size (d = 0.46), and higher drug consumption (p = .012) with a small effect size (d = 0.04), as shown in Table 3.
Table 3
Differences in variables between boys and girls
Hypothesis H3 was supported: the schoolchildren with PTSD had more sleep disruptions. The PTSD group had memory impairments and difficulty concentrating.
Adolescents with PTSD often experience disrupted sleep (often due to a heightened state of alert and distressing nightmares or flashbacks), which in turn exacerbates memory and concentration difficulties by interfering with the brain’s ability to process traumatic experiences and consolidate memories. Poor sleep leads to increased difficulty concentrating and remembering.
The main consequences of post-traumatic stress disorder and depression
We found that 49.8% of schoolchildren did not complete the homework requested by their teachers, and 52.6% demonstrated poor academic performance. Difficulties in concentration were reported by 50.1% of participants, while 10.2% experienced memory impairments. In addition, 29.7% of schoolchildren reported suicidal thoughts, and 29.3% expressed disinterest in daily activities.
Schoolchildren who engaged in truancy were at a higher risk of developing PTSD compared with those who did not (p = .041), with a moderate association (Cramer’s V = 0.33). Similarly, students who had repeated a grade were more likely to experience PTSD than those who had not (p = .032), also with a moderate association (Cramer’s V = 0.36). Furthermore, boys were more likely than girls to have repeated a grade (p = .045).
Schoolchildren who used tobacco were at higher risk of PTSD compared to non-users (p = .047), with a moderate association (Cramer’s V = 0.32), and the same was observed for drug consumption (p = .048), with a moderate association (Cramer’s V = 0.31).
Schoolchildren who experienced more traumatic events were at higher risk of PTSD compared to those who experienced fewer traumatic events (p = .028), with a strong association (Cramer’s V = 0.53), and girls had more traumatic events than boys (p = .032). Hypothesis H1 was supported: schoolchildren who used tobacco and drugs were at higher risk of PTSD. Schoolchildren who experienced more traumatic events were at higher risk of PTSD.
There was no significant relationship between PTSD status and father’s work (p = 0.061) and mother’s work (p = .113), as shown in Table 4.
Table 4
Differences in variables according to presence of PTSD
It may be because substance use can be a form of self-medication for trauma symptoms. Experiencing trauma can increase vulnerability to substance use disorders. The more traumatic events an adolescent experiences, the higher their risk of developing PTSD. They may use substances such as tobacco or drugs to cope with the distress and anxiety associated with trauma and PTSD symptoms.
The average scores for memory (p = .004) and concentration (p = .003) difficulties were directly and significantly correlated with the average PTSD score.
The higher the level of PTSD, the greater the risk of suicidal ideation (p = .002).
The average scores for depression (p < .001) and anxiety (p < .001) were directly and significantly correlated with the average PTSD score.
The higher the level of PTSD, the more the schoolchildren showed disinterest in activities (p = .003), as shown in Table 5.
Table 5
Correlations between the different variables and PTSD
| Level of anxiety | Level of depression | Memory difficulties | Level of concentration | Suicidal ideation | Disinterest in activities | |
|---|---|---|---|---|---|---|
| PTSD | ||||||
| r | .28 | .21 | .18 | .15 | .12 | .14 |
| p | < .001 | < .001 | .004 | .003 | .002 | .003 |
Hypothesis H3 was supported: the higher the level of PTSD, the more schoolchildren experience suicidal ideation. The higher the level of PTSD, the more the schoolchildren showed disinterest in activities.
Adolescents suffering from PTSD, particularly those experiencing symptoms such as intrusive thoughts, anger, and feelings of hopelessness and entrapment, may be at an increased risk of suicide. Additionally, PTSD can lead to emotional disengagement, which may result in a loss of interest in activities.
Discussion
Post-traumatic stress disorder (PTSD) was the primary focus of this investigation, which aimed to measure its prevalence among adolescents. The study was conducted in public middle schools in the city of Salé, Morocco. The results revealed that 42.7% of adolescents met the criteria for PTSD, while 57.3% did not exhibit symptoms of the disorder. A gender difference was observed, with 28.4% of affected participants being boys and 71.6% being girls. Regarding comorbid conditions, 91.3% of schoolchildren with PTSD also experienced anxiety, and 66.6% presented with depression, highlighting a strong association between PTSD and these disorders. Furthermore, 65.6% of schoolchildren with PTSD demonstrated poor academic performance.
More studies have concerned adults (Josse, 2011; Nixon et al., 2004; Pederson et al., 2004) compared to adolescents. It is only recently, during the last few years, that more such studies have been performed. Compared to adults, there is little specificity regarding the symptoms in adolescents, and in general, there is a great similarity between adolescent and adult PTSD symptoms. Schoolchildren are characterized by psychological and social specificities (adventure, the sense of discovering the world, the search for autonomy through contribution to their parents, etc.), and according to various studies this is why these adolescents may experience more traumatic events than adults (Christoffersen & Thorup, 2024; Nooner et al., 2012). Regarding exposure to at least one traumatic occurrence, the prevalence ranged from 40% to 90% and was even close to 100% (Costello et al., 2002; Elklit & Petersen, 2008). In a few studies in schoolchildren, the most observed traumatic event concerns the abrupt and unexpected death of a loved one (Halaly et al., 2024; Keyes et al., 2014; Mbwayo et al., 2019).
The adolescents were more likely to develop PTSD for several possible reasons, such as belonging to developing countries with low income like the country where our survey was conducted (Alzaghoul et al., 2022; Chossegros, 2011; Melese et al., 2024). Adolescents are at greater risk of developing PTSD, compared to adults, and the prevalence of this disease can vary from 5 to 90% (Alkharashi et al., 2022; Astitene & Barkat, 2021; DeVries & Olff, 2009). This difference in prevalence was due to certain factors such as the tools used to evaluate PTSD, the nature of the trauma, the age of the patient, the nature and culture of the population of the country of investigation, etc. (Brewin et al., 2025; Hodges et al., 2013).
In addition, sensitive schoolchildren, who are in a critical period in terms of emotional and behavioral regulation, were less well prepared to cope with a traumatic occurrence, which is why they were more likely to develop PTSD (Nooner et al., 2012; Tamir et al., 2025). Several studies show that boys experience more traumatic events than girls (Astitene et al., 2020; Craig & Sprang, 2014; Novotney, 2024).
However, several studies have shown that girls developed PTSD more frequently than boys (Astitene & Barkat, 2022; Borst et al., 2024; Craig & Sprang, 2014; Novotney, 2024).
Immediately after a traumatic experience, if not treated properly, many researchers address the issue of school and academic difficulties in schoolchildren. Children who have experienced traumas also often have relationship problems with peers and family members, problems with acting out, and problems with school performance (Koslouski et al., 2023; Zhao et al., 2024). Difficulties concentrating, memory loss, behavioral problems as well as disturbed sleep and adopting risky behaviors were also part of the difficulties of PTSD, along with impaired academic performance (Astitene & Barkat, 2021; Du et al., 2022; Sanger et al., 2025; Tuicomepee & Romano, 2008), which may increase the risk of repeating grades.
Various researchers have found that PTSD can cause an individual to have suicidal thoughts (Fox et al., 2021; Jannini et al., 2023), and especially in adolescents to use drugs, alcohol and tobacco excessively (Basedow et al., 2022; Brown et al., 2003; Kihas et al., 2024).
PTSD was very frequently encountered in the presence of comorbid psychopathological disorders such as anxiety and depression; these disorders may contribute to the intensity and maintenance of PTSD symptomatology (Assmann et al., 2021; Hicks et al., 2024; Wang et al., 2023). Compared to adults, young people were more vulnerable to anxiety and depression (Anderson et al., 2025; Kerig & Becker, 2010; Xiang et al., 2024).
Regarding our study, schoolgirls were more affected by comorbid disorders than schoolboys. Girls with PTSD exhibited higher rates of associated anxiety and depressive symptoms compared with boys. This finding aligns with previous research indicating that girls tended to have associated anxiety or depressive disorders more than boys (Konrad et al., 2022; Korte et al., 2021; Walter et al., 2022; Wamser-Nanney & Cherry, 2018).
All three hypotheses were supported:
H1: girls had a higher risk of PTSD compared with boys. The group without PTSD was older than the group with PTSD. Schoolchildren who used tobacco and drugs were at higher risk of PTSD. Schoolchildren who had more traumatic events were at higher risk of PTSD.
H2: The prevalence of anxiety and depression was higher in the group with PTSD than in the group without PTSD.
H3: The schoolchildren with PTSD had more sleep disruptions. The PTSD group had memory impairments and difficulty concentrating. The higher the level of PTSD, the more the schoolchildren experienced suicidal ideation. The higher the level of PTSD, the more the schoolchildren showed disinterest in activities.
The results obtained from PTSD assessments (the presence of PTSD symptoms such as intrusions, avoidance, and hyperarousal, as well as difficulties with emotional regulation, memory, and attention) have major practical significance and are crucial for comprehensive intervention:
For mental health professionals, they guide the diagnosis, assessment, and understanding of the severity of trauma and PTSD. They help determine the most appropriate therapeutic approaches, such as cognitive-behavioral therapy (CBT) or eye movement desensitization and reprocessing (EMDR).
For educators, these results can explain learning or behavioral difficulties. They can adapt their teaching methods to support students by taking into account their challenges with concentration, memory, or emotional regulation. Educators can also identify signs of psychological distress and refer students to appropriate support services.
For policymakers, PTSD results highlight the importance of investing in prevention strategies and early intervention following traumatic events. They justify the implementation of mental health support programs in schools and communities affected by major events.
The findings of this research on PTSD tend to extend and refine existing psychological models and enrich current theoretical frameworks. Our research aims to dissect and understand the processes and mechanisms that lead to the development of PTSD, particularly intrusive memories and avoidance behaviors.
This research continues to confirm and expand theories on how memory is affected by traumatic events, explaining why memories can resurface involuntarily and disruptively. The study of PTSD helps identify both risk and protective factors, thereby refining models of vulnerability and resilience in the face of trauma.
Our study of PTSD does not necessarily contradict existing psychological models; rather, it enhances them by providing valuable empirical data that allow for a more nuanced understanding and more effective applications.
The findings of the current study highlight the need for urgent public interventions from government and nongovernmental organizations to manage PTSD. Trauma-focused psychotherapies have the most empirical support for children and adolescents.
The results of this study could be used by governmental and private organizations to establish a support project for adolescents with psychological difficulties. It is strongly recommended to consider a program of support at school level provided by psychologists, which has not been implemented so far. Given the high prevalence of PTSD observed in this study, reliable and effective interventions are needed to address and treat this disorder. The most commonly used treatments for PTSD in adolescents include:
CBT (cognitive behavioral therapy): Trauma-focused cognitive behavioral therapy focuses on the relationship among thoughts, feelings, and behaviors; targets current problems and symptoms; and focuses on changing patterns of behaviors, thoughts and feelings that lead to difficulties in functioning. The patient needs to remember that avoidance of images or situations recalling the event acts as a factor in maintaining PTSD.
EMDR (eye movement, desensitization and information reprocessing): EMDR is a psychological therapy that aims to help a person integrate their memories of a traumatic event. It involves evoking distressing images, beliefs, and bodily sensations related to the trauma, while the therapist guides the patient's bilateral eye movements. The goal is to identify more positive perceptions of the trauma memories, to replace those that cause problems.
Also, psychoeducation and pharmacotherapy.
The treatment strategy should encompass psychological assessment and support; treatment includes behavioral therapy and sometimes selective serotonin reuptake inhibitors or antiadrenergic medications to hope for partial or complete remission of PTSD.
The intervention of public and private organizations is needed to support these adolescents to avoid school failure, which is a big national problem.
It is necessary to integrate specialists in the psychological field at the level of educational institutions. These specialists should be well trained in evidence-based interventions such as CBT and EMDR. Ideally, medical teams with solid training in CBT and EMDR should conduct regular visits to these institutions to provide ongoing assessment and therapeutic support.
In Morocco, the major obstacle to the absence of these specialists is the lack of funding and also a lack of awareness of the seriousness of PTSD. Potential solutions that can be suggested include awareness-raising by academics and researchers at the governmental and parliamentary levels on the importance of integrating specialized psychology teams into schools, and awareness-raising on the serious consequences of traumatic events on the well-being of schoolchildren at the academic and personal level.
Therefore, it is necessary to establish an action plan to promote the quality of life at the psychological and educational level by the national institutions concerned. Listening cells should be set up at school and those working in the field of mental health trained to contribute to the identification of learners at risk and enable the provision of support, including through referral systems to the health and social care sectors. Integrating mental health professionals into school systems could help identify and address PTSD symptoms early. With high rates of trauma exposure among schoolchildren, the need for intervention programs is clear. Delivery of such programs in the school setting eliminates key barriers to access to identify and address PTSD (Amin et al., 2020; Clarke et al., 2023; Phung, 2022).
The consequences of PTSD for the well-being of schoolchildren are serious. This causes great financial losses for the patient and for the nation. Therefore, the financial expenditure for public and private organizations will be justified and less than the expenditure needed to address PTSD.
The results of this study could be utilized by the government to set up a project to support adolescents with psychological difficulties. Training or strengthening of mental health skills is needed for school-based professionals interacting with children (teachers, educators, social workers, etc.) to address PTSD symptoms early. Direct access to a crisis support hotline on the schoolchildren portal for immediate assistance in case of an emergency is required (24/7 Helpline Integration). Programs (to address PTSD) to date have been designed for delivery by clinicians, who are a scarce resource in many schools. We can highlight a program that can be implemented successfully by teachers and school counselors, with good satisfaction among schoolchildren and parents, especially since those intervening have good knowledge of Morocco’s specific social, cultural, and economic landscape. With a promising program, one can reduce symptoms of PTSD among schoolchiImmediate post-care should be provided to patients who require it, and when necessary, they are referred to an appropriate follow-up or monitoring system. Psychological support should be offered promptly to minor victims and, when needed, to their parents. The adolescent psycho-trauma intervention team is composed of specialists in child psychiatry, clinical psychologists, nurses, and school-based psychiatric nurses, ensuring that affected adolescents receive comprehensive and professional care.
An agreement should be provided that includes the terms of provision of assigned health personnel and professionals for all or part of their activity. In addition, it should provide for the terms of compensation for mobilized personnel and professionals (travel, accommodation, etc.).
To understand the impact of long-term PTSD symptoms on educational and social outcomes during the course of studies at the level of Moroccan schools, it is necessary to conduct longitudinal studies to track the progression of PTSD among schoolchildren.
To compare and validate the results of these studies, it is advisable to expand different surveys that will be conducted in different regions of Morocco. This is why we encourage academic researchers to conduct these surveys.
Future research and limitations
Longitudinal studies would allow for a better understanding of how PTSD symptoms evolve over time. Expanding the sample size would strengthen the external validity of the results and better represent the diversity of traumatic experiences. It would also help to examine variations based on age, gender, and socio-cultural context. Future studies should also incorporate additional variables, including biological and neurophysiological factors, contextual and environmental variables, as well as cognitive and emotional components.
Most diagnostic tools and theoretical models of PTSD have been developed in Western contexts, which may limit their relevance in other cultural settings. Standardized questionnaires may not be suitable for all populations. The wide variety of cultural perspectives makes it difficult to develop universally applicable models of PTSD.
There is also a difference in access to mental health services and in the willingness to share traumatic experiences among individuals who participate in PTSD studies. When samples are limited (in size, cultural diversity, or access to care), it becomes difficult to generalize findings to broader populations. Additionally, there is variation in how PTSD is defined and diagnosed across different healthcare systems.
Conclusions
PTSD is a reaction to traumatic events that can have significant physical, functional, and psychological effects on the daily life of adolescents. Our investigation elucidated a complex interplay of factors contributing to the emergence of PTSD following trauma.
Gender, residential environment (poverty, social precariousness, high unemployment, and an unclear vision of the future), geographical location (Morocco is a low- to middle-income countries), educational attainment (a high rate of parental illiteracy), family support (a lack of social support), and the nature and locus of the trauma were revealed as integral elements in this disorder.
To reduce the negative psychosocial, economic, and health problems, the results of our study must be taken into consideration by local Moroccan authorities to improve the quality of life of these schoolchildren.