BACKGROUND
Health-related quality of life (QoL) has become an essential endpoint in medical and health research (Haraldstad et al., 2019). Even though achieving a good QoL is a worthy goal in its own right, in the context of medical services, monitoring patients’ well-being is an integral part of strategies proposed to promote adherence to medical regimens (Bosworth, 2006). Adherence to physician’s prescriptions and recommendations acts as a potent mediator between medical practice and patient outcomes, and non-adherence can become a rational choice if the patient feels that their well-being and quality of life are being compromised (Naber & Karow, 2001; Ogden, 2016). In reproductive medicine, in particular, it has been demonstrated how greater regard for the psychological distress patients may experience before and during treatment can improve treatment compliance and reduce drop-out rates (Verberg et al., 2008).
Over the past decade, there has been an increased focus on fertility-related QoL (Boivin et al., 2011a) and the psychosocial and psychosexual well-being of individuals and couples who are in assessment for infertility and/or are in the process of undergoing assisted reproductive technology procedures (e.g., Arpin et al., 2019; Chamorro et al., 2023). Patients with clinical infertility, which has been defined by the World Health Organization (WHO) as “a disease of the reproductive system defined by the failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse” (Zegers-Hochschild et al., 2009), tend to report a wide array of psychosocial and psychosexual issues (Chachamovich et al., 2010; Luk & Loke, 2015; Thoma et al., 2021). These may include infertility-related emotional problems such as anxiety, depression, and general distress (Massarotti et al., 2019; Öztekin et al., 2020), as well as impaired sexual functioning (Coşkuner Potur et al., 2020; Lotti & Maggi, 2018). Such challenges can affect not only an individual’s well-being but also that of the partner (Nakić Radoš et al., 2022), the couple’s relationship (Luk & Loke, 2019), and broader social relations, including the most extreme repercussions, such as emotional, verbal, and even physical violence (Çambel & Akköz Çevik, 2022; Wang et al., 2022). In women, QoL is compromised in both primary infertility (defined as infertility in a woman who has never had a clinical pregnancy) and secondary infertility (infertility in a woman who has had at least one clinical pregnancy) (WHO, 2023), but more so in the former (e.g., Karabulut et al., 2013). Also, women in couples where the cause of infertility involves both partners exhibit more significant infertility-related distress than those who are fertile but whose partner is not (Yilmaz et al., 2020). Furthermore, those who have been infertile for a more extended time experience greater severity of infertility-related adverse effects (Karabulut et al., 2013). The process of treatment itself may generate additional distress. For instance, Szigeti et al. (2022) found that being in treatment for infertility was associated with poorer emotional and physical, cognitive, and behavioral outcomes on a widely used fertility-related QoL measure, FertiQoL (Boivin et al., 2011a), relative to the pre-treatment status. Although men’s QoL is also affected by infertility itself (Makara-Studzińska et al., 2022) and infertility treatment (Peronace et al., 2007), at least some of the impacts of infertility are felt more heavily by women (Casu & Gremigni, 2016; Chachamovich et al., 2010; Luk & Loke, 2019; Onat & Beji, 2012; Zurlo et al., 2018). Some studies did not show any gender differences (e.g., Antequera-Jurado et al., 2024), which may be partly attributable to the fact that scores of unrelated individuals were compared in previous studies (e.g., Antequera-Jurado et al., 2024).
Besides gender, another array of factors modulating QoL in infertility involves socioeconomic status. There is evidence in non-Western countries that health-related psychological distress in infertile women differs according to their education, employment, and income (Chachamovich et al., 2007; Karabulut et al., 2013; Namdar et al., 2017; Yilmaz et al., 2020). However, in less traditional, more egalitarian sociocultural contexts, the effects of sociodemo-graphic variables on fertility-related QoL may be much weaker (van Rooij et al., 2007; Vanderlinden, 2009). The evidence from European countries is limited. The research gap is particularly evident in Central and Eastern European countries (Mascarenhas et al., 2012). Moreover, researchers have focused predominantly on individuals rather than couples (Makara-Studzińska et al., 2022; Szigeti et al., 2022; Wdowiak et al., 2021) and on largely heterogeneous samples consisting of primary and secondary infertile individuals.
In the Czech Republic, specifically, infertility-related distress is uniquely shaped by the region’s post-communist cultural and historical background. In this secular country, distinguished by its advanced biomedical infrastructure and high standards of medical care, including assisted reproductive technology (ART) (Slepičková, 2022), parenthood remains a highly valued life goal, supported by persistent pronatalist norms (Hašková & Dudová, 2021; Sobotka, 2016). For a great proportion of Czech people, childbearing is perceived not merely as a choice but as a natural and expected part of adult life (Kuźniar, 2024; Waldaufová & Šťastná, 2025). Infertility is often framed as a technical, biomedical failure to be managed by experts, intensifying the pressure on individuals to seek a cure through ART (Slepičková et al., 2012; Šmídová et al., 2015). Historically, in medical and media narratives surrounding conception and infertility treatment, women have been burdened with the primary responsibility for reproduction and positioned as culpable when they did not conceive (Dudová & Hašková, 2023). The post-communist transition has brought significant changes to fertility patterns among women (Kocourková et al., 2022; Slabá et al., 2024) as well as men (Kyzlinková & Šťastná, 2018), driven by shifts in cultural values, attitudes, and behaviors (Chromková Manea & Rabušic, 2019; Polesná & Kocourková, 2016) and the increased availability of contraception (Kocourková & Fait, 2011). The postponement of fertility, as evidenced by the consistent increase in the average age of first childbirth from 1994 to 2015 (Fait et al., 2022), correlates with a higher reliance on ART (Kocourková et al., 2014; Kocourková & Fait, 2009). For women under the age of 40, health insurance companies cover basic services for three in vitro fertilization (IVF) cycles with embryo transfer. If only one embryo was transferred in the first two cycles, a fourth cycle is also covered (Crouch, 2025). While intended to alleviate reproductive difficulties, the wide availability of ART can paradoxically impose novel forms of social and psychological pressure. Women in particular may experience a growing sense of urgency to conceive at all costs, partly because the clinical environment – through both direct encouragement and indirect suggestion – may promote the idea that as long as there is hope, they are obligated to continue treatment (Slepičková, 2015). Women also generally report higher levels of stress than men in response to infertility and failed ART procedures (Davidová & Pechová, 2014). Despite the age-related decline in fertility, the increased incidence of fertility-impairing conditions, and the higher risk of pregnancy loss (ASRM, 2014), women’s age and the number of years of infertility were not found to be statistically significant predictors of life satisfaction in a previous Czech sample (Ďurašková et al., 2016).
Several studies conducted in Central European samples showed mixed results regarding associations between sociodemographic variables and FertiQoL scores. For example, in Hungarian women, Szigeti et al. (2022) found that being older was correlated with higher FertiQoL emotional scores and that living in a village (rather than in a larger place) was associated with higher core and social scores. The rest of the sociodemographic and medical variables, such as education, cause of infertility (female factor/male factor/both/unexplained), duration of efforts to conceive, and relationship length, did not show any associations with FertiQoL scores. On the other hand, in Polish women and men, education did affect total FertiQoL reports positively, and trying to conceive for a more extended time was associated with poorer scores (Makara-Studzińska et al., 2022; Wdowiak et al., 2021).
The objective of the present study was to identify the sociodemographic and medical correlates of fertility-related quality of life of couples living with primary infertility in the Czech Republic, which remains a lesser-researched Central European region. The strict focus on primary infertility was intended to obtain a more homogeneous sample, as already having a child appears to be one of the strongest positive influences on FertiQoL scores (Szigeti et al., 2022). Since the Czech Republic is among the countries with the lowest inequality in income distribution worldwide (Makreshanska-Mladenovska & Petrevski, 2019), and in general, the QoL in a Czech municipality is not a function of its size (Petrovič & Maturkanič, 2022), in this multicentric study we hypothesized that the sociodemographic variables of education, municipality, and net income of the couple’s household would not affect FertiQoL scores. However, we expected that the FertiQoL outcomes would be influenced by gender both as a main effect and in interaction with age and cause of infertility (female/male/mixed/unexplained), respectively. Regarding the gender*age interaction, research shows that the repercussions of unwanted childlessness tend to disproportionately burden older women compared to younger women and men (e.g., Greil et al., 2011; Zurlo et al., 2018). As regards the gender*cause interaction, the findings are less clear. The intuitively appealing notion is that the presence of a female factor in women (e.g., Kulaksiz et al., 2022) and a male factor in men (Asazawa et al., 2019) would be associated with worse psychosocial and QoL outcomes than in their same-gender peers with a different infertility factor. However, some studies have found the opposite, with women in malefactor cases and men in female-factor cases showing poorer outcomes (e.g., Vizheh et al., 2015). Therefore, regarding the cause of infertility, we did not formulate any specific hypotheses and merely explored its effect on FertiQoL scores. Furthermore, since failed past infertility treatments have been reported to affect women’s and men’s QoL negatively (Lee et al., 2010; Peronace et al., 2007; Yamanaka-Altenstein et al., 2022), we expected to find a negative effect of having undergone any ART procedures in the past. We were also interested to know whether past ART exposure differentially affected women’s and men’s FertiQoL scores and whether its impact differed in couples according to cause of infertility. Also, a longer duration of efforts to conceive (whether in general or with ART) was hypothesized to be associated with poorer FertiQoL scores (Makara-Studzińska et al., 2022; Wdowiak et al., 2021), whereas the length of relationship was not expected to play a significant role (Szigeti et al., 2022). Since the attributes and behaviors of one partner can affect the outcomes of the other partner, we implemented the Actor-Partner Interdependence Model (APIM) (Kashy & Kenny, 2000), which uses the dyad (couple) as the unit of analysis. In so doing, we employed hierarchical linear modelling (Campbell & Kashy, 2002), which is rarely used in infertility research.
PARTICIPANTS AND PROCEDURE
PARTICIPANTS
Respondents in this study were 469 primary infertile Czech couples. Women had never been pregnant, and their male partners were childless. Women’s mean age was 30.79 ± 4.65, 20-48 years, and men were on average 33.19 ± 4.94, 21-52 years old. On average, women were two years and five months younger than their partners (SD = 4 years 4 months; range: 23 years younger to 14 years older). The ages of both partners were positively associated (r = .60, p < .001). Based on published recommendations on sample size calculation (e.g., Jones et al., 2003) and previous studies that used the FertiQoL measure (Boivin et al., 2011a, 2011b), we computed the number of couples we needed to approach. Precisely, with SDs of FertiQoL domains ranging from as low as 9.39 in Cserepes et al. (2014) to up to 23.7 in Sexty et al. (2016), a power level (pβ) of 0.90, and the objective of detecting a minimum of a 10-point difference between the various sociodemographic groups, the N needed to test a two-sided hypothesis was calculated to be 328 (2 × 164). Accounting for a response rate that could range from as low as around 60% (Chan et al., 2019) to as high as nearly 100% (Jacob et al., 2021), we approached 550 couples through four clinics of human assisted reproduction. The clinics were based in the following regions of the Czech Republic: Moravian-Silesian (Reprofit International Ostrava; n = 314; 67%), South Moravian (Reprofit International Brno; n = 112; 23.9%), Olomouc (IVF Clinic; n = 22; 4.7%), and Prague (Gennet; n = 21; 4.5%). The overall response rate was 85.3% (n = 469).
The present study was part of a broader project on psychosocial and psychosexual functioning in couples living with primary and secondary infertility. The data collection took place between July 2020 and February 2022. The study protocol was approved by the Bioethics Committee of the Clinic of Reproductive Medicine and Gynaecology Reprofit, Approval No. 2020/020. All the participants provided preliminary verbal and written informed consent. The procedures were in accordance with the 1975 Declaration of Helsinki, as revised in 2008. The respondents or medical professionals did not receive any financial or other reimbursement for their participation in the study.
SURVEY TOPICS
Sociodemographic and medical variables. The survey consisted of 77-item female, 65-item male, and 9-item medical professionals’ forms, which are appended in the Supplementary Material. For the present study, we surveyed each partner about their age, education, and relationship length. Furthermore, women were asked to indicate how many years and months they had been trying to conceive (in total and specifically with ART). Men were requested to provide information on the size of the couple’s current place of residence (municipality) and the net income of the couple’s household. Length of the relationship and efforts to conceive (in total and with ART) were converted to months, and women’s and men’s estimates of the relationship length were averaged. Also, due to low counts, education categories of primary education and PhD or higher academic rank were merged with the next higher and lower categories, respectively. For the same reason, the two income categories upwards of CZK 75,000/month were merged. The reproductive physician who was in charge of the given couple’s treatment was asked to indicate the cause of infertility (female factor/male factor/mixed/unexplained), each partner’s medical history, and how many intrauterine inseminations (IUIs), in vitro fertilization and embryo transfers (IVF ETs) and cryoembryotransfers (CETs) the couple had already undergone and whether there were any ART procedures planned for them. Table 1 shows the mean ± SD for continuous variables and the categories and their absolute and relative frequencies for ordinal variables.
Fertility-related quality of life. The FertiQoL instrument is the first internationally validated questionnaire to measure QoL in individuals experiencing fertility problems. It consists of the 24-item core module and an optional 10-item treatment module not administered in the present study. The core module comprises four subscales with six items per subscale: Emotional, Mind-Body (MB), Relational, and Social. The Emotional subscale score reflects the negative emotions’ effect on QoL. The MB subscale refers to how fertility issues affect the individual’s physical health, cognitive functioning, and everyday behaviors. The Relational subscale score represents the impact of fertility issues on various aspects of the marital or romantic relationship. Finally, the Social subscale score conveys the consequences of fertility problems for social interactions. Sample items include “Do your fertility problems cause feelings of jealousy and resentment?” (Emotional), “Do you think you cannot move ahead with other life goals and plans because of fertility problems?” (MB), “Have fertility problems strengthened your commitment to your partner?” (Relational), “Do you feel social pressure on you to have (or have more) children?” (Social). All items use a 5-category response format, but the categories differ depending on item content (e.g., very poor/poor/neither poor nor good/good/very good; always/very often/quite often/seldom/never). Scores range from 0 to 4. Reverse items are recoded, and items are summed and scaled to range from 0 to 100. Higher subscale scores suggest better QoL. In addition to the subscale scores, two single items regarding general physical health (“How would you rate your health?”) and satisfaction with QoL (“Are you satisfied with your quality of life?”) are rated using a 5-category response format. Internal reliability of the Core FertiQoL and its subscales ranged from .63 to .92 in European samples (Aarts et al., 2011; Cserepes et al., 2014; Lopes et al., 2014; Pedro et al., 2013). For this study, we used the Czech translation of the FertiQoL questionnaire. It is important to note that, at the time of this research, there was no published study on the formal validation or cultural adaptation of the FertiQoL for the Czech population. The existence of the Czech translation is only implied by a short note in the Funding section of the Koert et al. (2021) paper. It is not advertised on the website of the corresponding author’s institution as available for download (https://sites.cardiff.ac.uk/fertiqol/download/). As researchers are advised not to create their own translations, the official Czech version was obtained through personal communication with one of the tool’s original developers, Dr. Jacky Boivin.
Table 1
Descriptive statistics of the sociodemographic and medical variables in couples with primary infertility (N = 469)
We assessed the internal consistency of the sub-scales using Cronbach’s alpha (α) to establish the measure’s reliability in our sample. For the total sample, the Mind-Body (α = .86) and Emotional (α = .84) subscales demonstrated good internal consistency, while the Relational (α = .64) and Social (α = .62) sub-scales showed acceptable consistency (Forero, 2014). A gender-specific analysis revealed that reliability was generally higher for women. The Mind-Body and Emotional scales maintained good consistency for both women (α = .87 and .85, respectively) and men (α = .79 and .76, respectively). The Relational and Social scales remained in the acceptable range for both women (α = .63 and .64, respectively) and men (α = .64 and .60, respectively).
PROCEDURE
Medical doctors with a specialty in reproductive medicine were instructed to ask the couple to complete two gender-specific survey sheets (a female and a male form) at the end of the appointment. The survey sheets were distributed predominantly at first-time appointments for treatment consideration or consultation and completed in the clinic’s waiting room. The patients were informed that the survey would take about 15 minutes. When both the partners were interested in participating, the doctor presented them with the two forms, explained the significance of the study and its outcomes, assured them of the anonymity of their responses, informed them that they could withdraw from the study at any time, and answered any questions. If both the partners had given their written consent to take part in the study, they were asked to complete the two gender-specific forms in the waiting room. The participants were instructed to refrain from consulting their responses with their partners. They put the completed forms in unmarked envelopes and submitted them to a designated box in the waiting room next to the reception. The physicians then completed a third form, labelled with the couple’s ID, to provide the necessary medical information. The respondents or medical professionals did not receive any financial or other reimbursement for their participation in the study.
STATISTICAL ANALYSIS
Exploratory chi-square, t-tests, and Pearson correlations were conducted using IBM SPSS 26.0 software. Dyadic multilevel modelling was performed with SAS Studio 3.82 (Enterprise Edition) via SAS OnDemand for Academics. The APIMs were fitted with PROC MIXED. To fit APIMs, we closely followed the guidelines published by Campbell and Kashy (2002). Assumption verification, data model specification and estimation, and model-data agreement assessments were further guided by the recommendations of Bell et al. (2013) and Wickham and Knee (2012). Scaling and categorization of the independent variables (IVs) that were entered as main effects or in interactions to provisional candidate models can be found in Table 1. Actor effects (i.e., effects of a person’s IVs on their own FertiQoL scores) and partner effects (i.e., influences of their IVs on their partner’s FertiQoL scores) were modelled for age and education, which were the mixed predictor variables (i.e., variables for which there was variation both within and between dyads). Gender was a within-dyad variable, while net household income, municipality size, relationship length, duration of efforts to conceive (with/without ART), ART status, and cause of infertility were between-dyad variables. Categorical variables (gender, education, net household income, municipality size, cause of infertility, and ART status) were effect-coded. The reference categories (coded with –1s) were as follows: female gender; secondary education; net monthly household income of CZK 46,000–60,000; municipality population of 50,000–200,000; female-factor cause of infertility; any prior ART exposure. The selection of female gender, female factor, and prior ART experience as reference categories was informed by the suggestions of Johfre and Freese (2021). They advise considering the relevance to policy when choosing a reference category, and also to select categories associated with lower predicted values, thereby ensuring a positive coefficient in the table. The reference categories for the net monthly household income and municipality population were selected to approximate the median values observed in the Czech population (CZSO, 2022a, 2022b). Specifically, assuming that both partners worked full time for the median gross monthly wage, they would earn a combined gross income of CZK 65,000–75,000 per month, which amounts to a combined net income of CZK 50,000– 58,000 per month. Furthermore, roughly half of Czech municipalities have populations under 500 people, while those classified as ‘medium-sized’ typically range between 2,500 and 5,000 residents. Quantitative predictor variables (age, relationship length, duration of efforts to conceive with/without ART) were grand mean-centered. Furthermore, we analyzed the effects of the absolute difference between both partners’ ages as well as the differential effect of age, cause of infertility, and ART with respect to gender (interactions: gender*age, gender*cause of infertility, gender*ART status) and ART with regard to cause of infertility (ART*cause of infertility). Multiple candidate models were fitted, and fit statistics were compared to produce the final models. From these, the duration of efforts to conceive (with/without ART) was omitted to obtain a better fit. Based on the recommendations of Kincaid (2005), an unstructured covariance (UN) structure was selected. The estimation approach was the default method of restricted maximum likelihood (REML).
RESULTS
GENERALIZED LINEAR MIXED MODELS
The Actor-Partner Interdependence Model (APIM) analyses (Tables 2-6) revealed significant main effects and interactions related to gender and medical history, which were further explored through post-hoc tests (Table 7). A significant gender effect was observed across almost all FertiQoL domains, with men reporting higher scores than women on the total, Emotional, Mind-Body, and Social subscales; the only exception was the Relational scale, where no significant gender difference was found. The mean within-couple difference in scores ranged from 5.5 points (Social scale) to 13.7 points (Emotional scale).
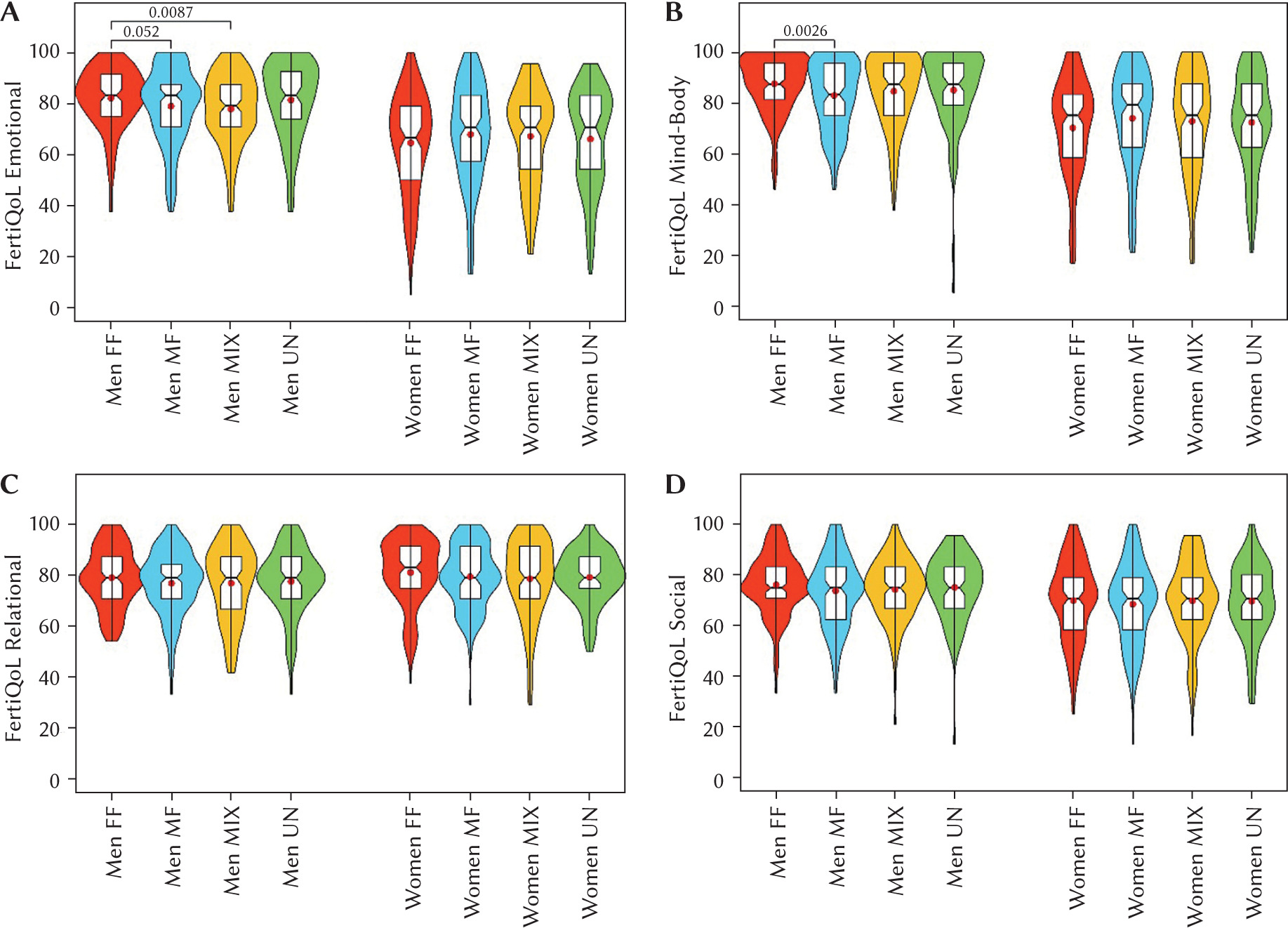
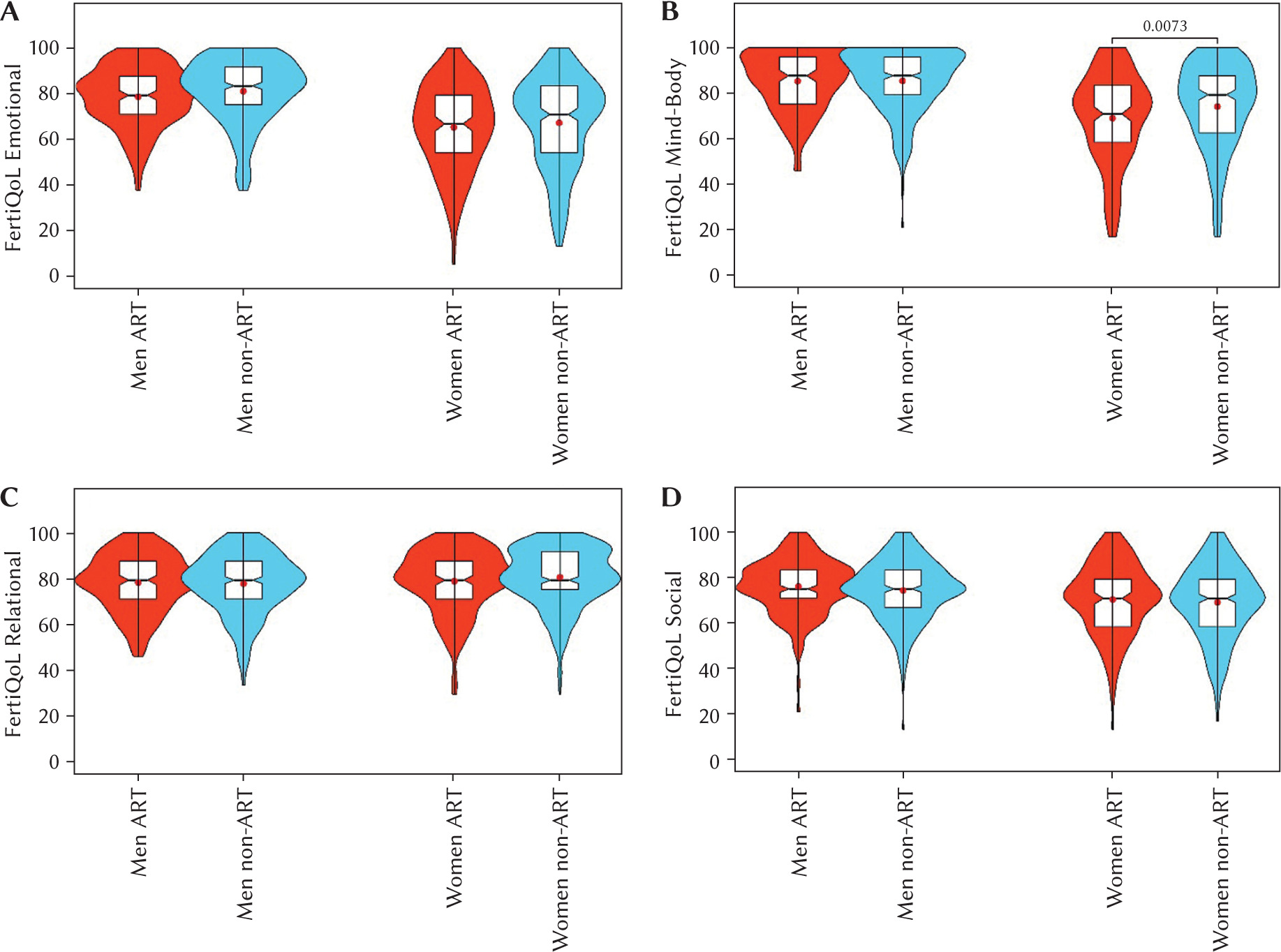
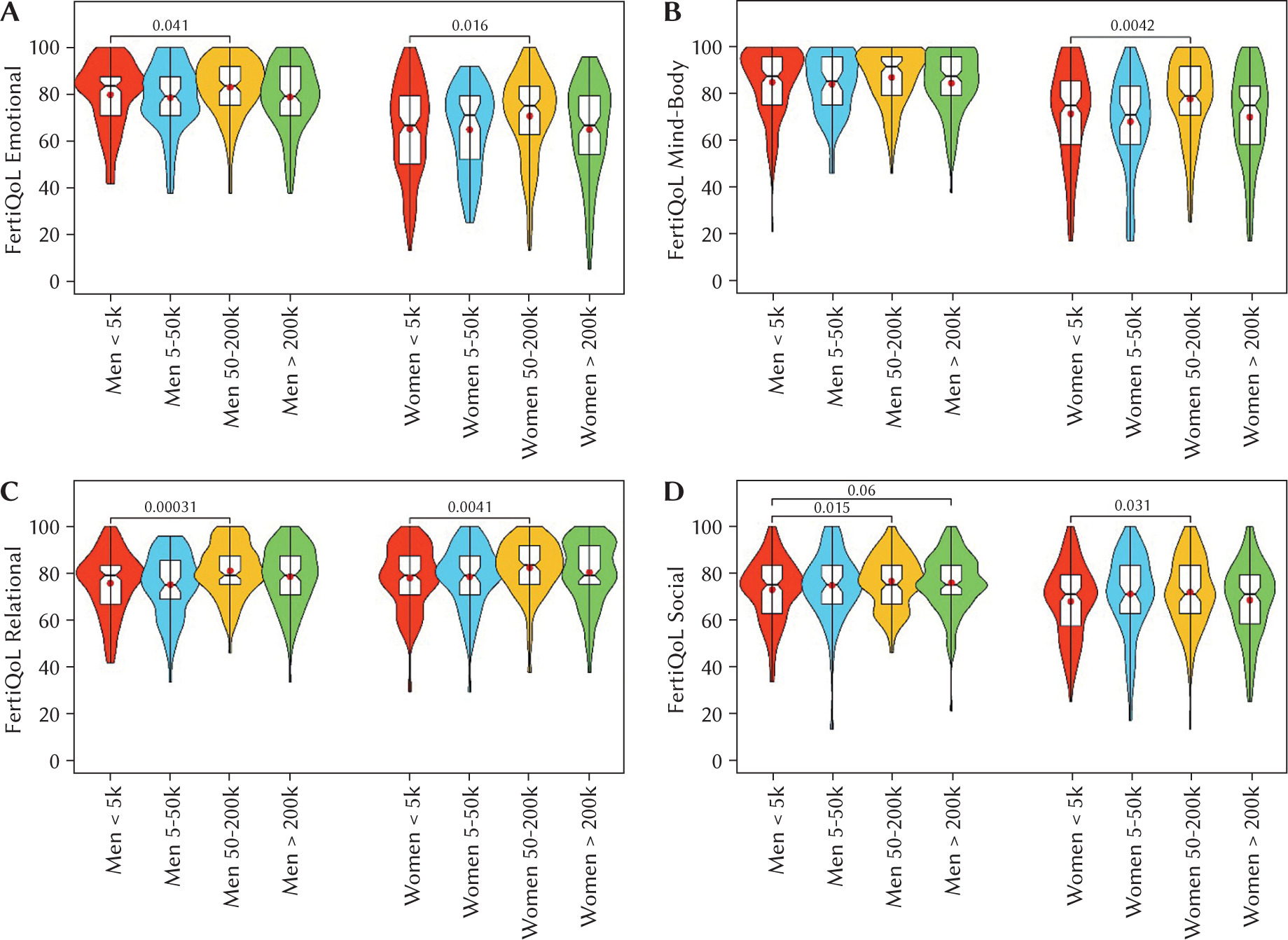
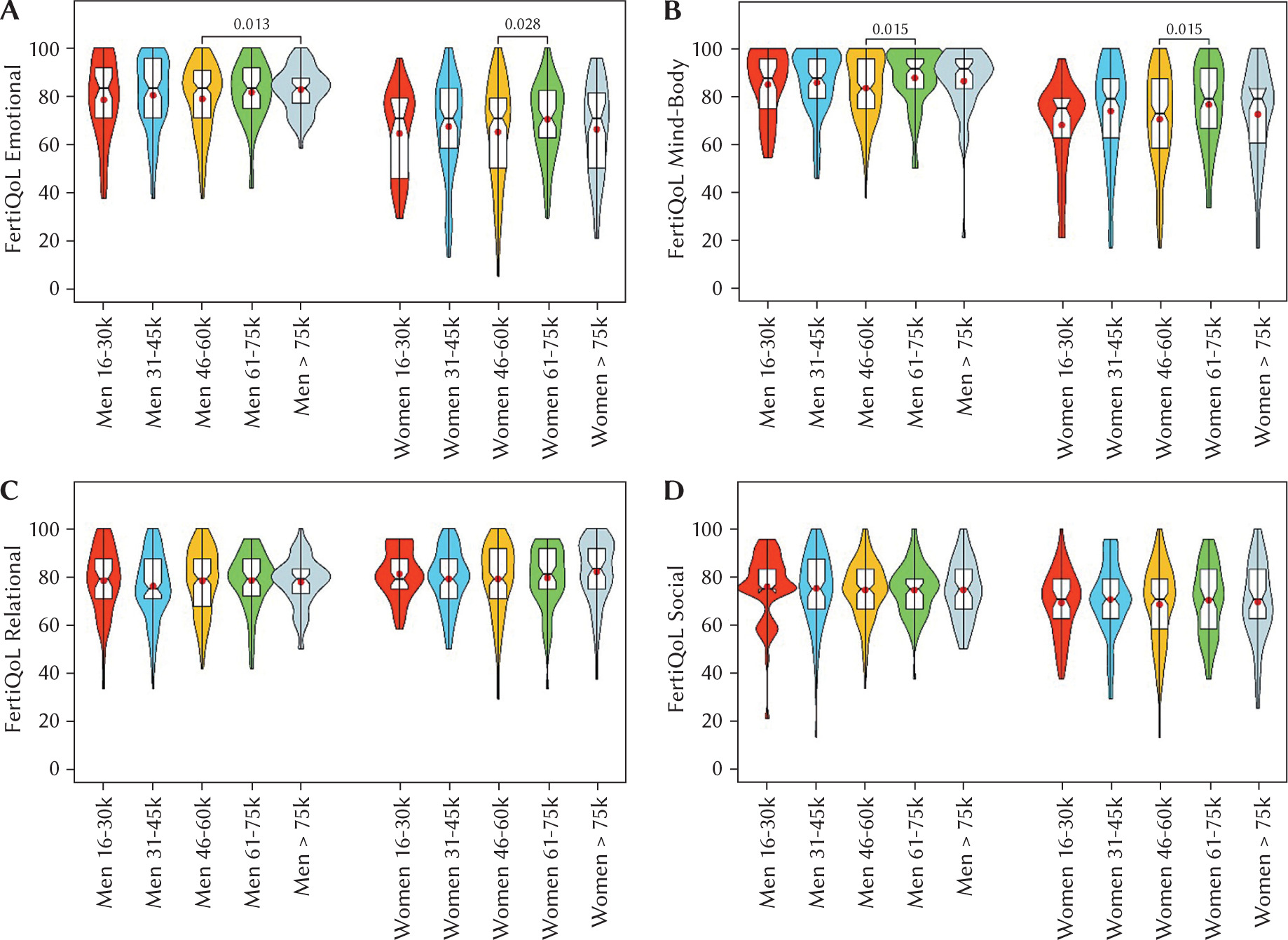
The diagnosed cause of infertility emerged as a significant moderator of quality of life, with effects contingent upon gender. Specifically, whereas women’s scores remained stable (i.e., consistently lower than men’s) across different etiologies, men reported significantly lower scores on the Emotional and Mind-Body scales when infertility was attributed to a male-specific versus a female-specific cause. As illustrated by exploratory analyses in Figure 1, this pattern extended to men in couples with mixed-factor infertility, who also reported lower Emotional scores. Similarly, prior experience with assisted reproductive technology (ART) was associated with diminished scores on the Emotional and Mind-Body scales. This effect was further moderated by gender for the Mind-Body scale; post-hoc analyses, detailed in Figure 2, indicated that only women with prior ART experience reported reduced scores, while no such effect was observed for men. Sociodemographic variables were also found to be significant, albeit inconsistent, predictors of FertiQoL outcomes. Municipality size demonstrated the most prominent influence. Individuals residing in cities with populations between 50,000 and 200,000 reported significantly higher FertiQoL scores across most domains compared to those in towns with fewer than 5,000 inhabitants. Although the primary model for the Social scale was not significant, exploratory analyses presented in Figure 3 revealed a similar advantage for residents of larger cities in this domain as well. The effect of household income was more circumscribed, with the primary APIM analyses indicating a significant positive association only with Mind-Body scores. Specifically, couples with a monthly income of CZK 61,000– 75,000 reported higher Mind-Body scores than those in the reference category of CZK 46,000–60,000. Exploratory findings presented in Figure 4, however, suggested that income may also influence Emotional scores. Finally, age and relationship duration showed distinct associations with quality of life. Age demonstrated a primarily positive, though limited, relationship with outcomes. An individual’s older age was positively associated with their own Emotional scores (an actor effect), and having an older partner was positively associated with Mind-Body scores (a partner effect). Conversely, a longer relationship duration was negatively associated with scores on the total, Relational, and Social scales.
DISCUSSION
In the present study we investigated how gender, fertility-related medical history, and sociodemographic factors interact to affect the fertility-related quality of life (FertiQoL) of treatment-seeking couples facing primary infertility. These variables were previously identified as affecting FertiQoL scores in other European samples (Makara-Studzińska et al., 2022; Szigeti et al., 2022; Wdowiak et al., 2021). Our findings confirm that gender is a critical determinant, with women reporting a significantly lower quality of life across the Emotional, Mind-Body, and Social domains than their male partners. This observation is highly consistent with a substantial body of research indicating that women often bear a disproportionate psychological burden of infertility (Assaysh-Öberg et al., 2023; Casu & Gremigni, 2016; Celda-Belinchón et al., 2025; Chachamovich et al., 2010; Dourou et al., 2023; Luk & Loke, 2019; Onat & Beji, 2012; Sexty et al., 2016; Zurlo et al., 2018). These effects were particularly marked in women with a female-factor diagnosis and those with prior ART experience. The gender effect in our sample can be interpreted from several perspectives. For many couples, especially those in the early stages of treatment, like a majority of our sample, the primary distress arises from the overt acknowledgment of their inability to conceive, which can be threatening particularly to women’s sense of self-worth and life satisfaction (Fieldsend & Smith, 2020; Grunberg et al., 2022). The direct confrontation with the sense of “disability,” coupled with anxieties about and actual experience with the demanding treatment process, the fear of failure, and maladaptive coping strategies such as self-blame, appears to impact women more profoundly (Ghorbani et al., 2025; Guštin et al., 2023; Langher et al., 2019). This is in part because the psychological, physical, and logistical brunt of medical intervention, which can be enormous (Courbiere et al., 2020; Gupta et al., 2024), falls upon them, regardless of etiology (Aiello et al., 2025; Domar et al., 2018). Advances in reproductive technology, while benefiting many, have inadvertently further concentrated the responsibility for achieving fertility on women (Carson et al., 2021; Kashyap & Tripathi, 2025), with most medical interventions being focused on the female body (Hal-comb, 2018). Even in cases of male-factor infertility, it is the woman who undergoes frequent monitoring, self-administers hormones, and endures invasive procedures (Kim et al., 2014), which inextricably links her body and psychological state to the treat-ment’s success or failure (McLaughlin & Cassidy, 2019; Nicoloro-SantaBarbara et al., 2018; Purewal et al., 2018). This distress is compounded by the notion that feeling stressed could, in itself, reduce the chances of successful treatment (Negris et al., 2021; Rooney & Domar, 2018).
Table 2
Solution for fixed effects of the APIM fitted to model the effects of sociodemographic and medical variables on total FertiQoL scores
[i] Note. APIM – Actor-Partner Interdependence Model; FertiQoL – fertility-related quality of life. Categorical variables were effect-coded, the reference category (ref; coded as –1) is given in brackets. SE – standard error, LL – lower limit, UL – upper limit. The actor effects of age and education mean how a person’s age and education affect their own FertiQoL score. The partner effects of age and education refer to how a person’s age and education affect their partner’s FertiQoL score. ART stands for assisted reproductive technology.
Table 3
Solution for fixed effects of the APIM fitted to model the effects of sociodemographic and medical variables on Emotional FertiQoL scores
[i] Note. APIM – Actor-Partner Interdependence Model; FertiQoL – fertility-related quality of life. Categorical variables were effect-coded, the reference category (ref; coded as –1) is given in brackets. SE – standard error, LL – lower limit, UL – upper limit. The actor effects of age and education mean how a person’s age and education affect their own FertiQoL score. The partner effects of age and education refer to how a person’s age and education affect their partner’s FertiQoL score. ART stands for assisted reproductive technology.
Table 4
Solution for fixed effects of the APIM fitted to model the effects of sociodemographic and medical variables on Mind-Body FertiQoL scores
[i] Note. APIM – Actor-Partner Interdependence Model; FertiQoL – fertility-related quality of life. Categorical variables were effect-coded, the reference category (ref; coded as –1) is given in brackets. SE – standard error, LL – lower limit, UL – upper limit. The actor effects of age and education mean how a person’s age and education affect their own FertiQoL score. The partner effects of age and education refer to how a person’s age and education affect their partner’s FertiQoL score. ART stands for assisted reproductive technology.
Table 5
Solution for fixed effects of the APIM fitted to model the effects of sociodemographic and medical variables on Relational FertiQoL scores
[i] Note. APIM – Actor-Partner Interdependence Model; FertiQoL – fertility-related quality of life. Categorical variables were effect-coded, the reference category (ref; coded as –1) is given in brackets. SE – standard error, LL – lower limit, UL – upper limit. The actor effects of age and education mean how a person’s age and education affect their own FertiQoL score. The partner effects of age and education refer to how a person’s age and education affect their partner’s FertiQoL score. ART stands for assisted reproductive technology.
Table 6
Solution for fixed effects of the APIM fitted to model the effects of sociodemographic and medical variables on Social FertiQoL scores
[i] Note. APIM – Actor-Partner Interdependence Model; FertiQoL – fertility-related quality of life. Categorical variables were effect-coded, the reference category (ref; coded as –1) is given in brackets. SE – standard error, LL – lower limit, UL – upper limit. The actor effects of age and education mean how a person’s age and education affect their own FertiQoL score. The partner effects of age and education refer to how a person’s age and education affect their partner’s FertiQoL score. ART stands for assisted reproductive technology.
Beyond this well-established gender difference, our study’s dyadic approach revealed crucial nuances based on the diagnosed cause of infertility. While women’s FertiQoL scores remained remarkably consistent regardless of the reason for infertility, men reported significantly lower Emotional and Mind-Body quality of life when the cause was attributed to a male-specific or mixed factor. This powerful interaction suggests that the psychological impact on men is not uniform but is amplified by the attribution of “responsibility” (Dooley et al., 2011). This finding may reflect deep-seated societal pressures and cultural narratives linking male fertility to virility and identity (Abbasi et al., 2025; Cervi & Knights, 2022; Hanna et al., 2025). In fact, a body of evidence suggests that societal perceptions of infertility tend to place a heavier stigma on male-factor causes than on other diagnoses (Wischmann & Thorn, 2013) because prevailing cultural narratives portray men as inherently fertile, disengaged from the parental role, and emotionally detached (Hanna & Gough, 2020). A male-factor diagnosis can thus be perceived as a direct threat to one’s masculinity, leading to heightened feelings of shame, self-blame, and distress (Arya & Dibb, 2016; Obst et al., 2023) that may manifest in lower quality of life scores.
Table 7
Overview of significant effects found in the APIM analyses for the individual and total FertiQoL scores and related post-hoc and exploratory analyses and descriptive statistics
[i] Note. APIM – Actor-Partner Interdependence Model; FertiQoL – fertility-related quality of life; ART – assisted reproductive technology. Within-couple gender differences in scores were computed by subtracting the female partner’s score from the male partner’s score. Between-category analyses (◊) were run for couples’ composite scores calculated by adding the scores of both partners together. Bias-corrected and accelerated bootstrap 95% confidence intervals are shown in brackets. SD – standard deviation, SE – standard error, † not accounting for the dependency between paired observations, ‡ paired sample t-tests, ns – non-significant,  statistically significant in APIM analyses, ♂+♀ sum of male and female partner’s scores, ♂-♀ difference between male and female partner’s scores.
statistically significant in APIM analyses, ♂+♀ sum of male and female partner’s scores, ♂-♀ difference between male and female partner’s scores.
Prior experience with assisted reproductive technology (ART) also emerged as a key moderator of well-being, particularly for women. Consistent with the abundant literature on the psychological toll of undergoing ART interventions (Domar et al., 2018; Haemmerli Keller et al., 2018; Kang et al., 2022; Öztürk et al., 2021), prior ART experience was associated with diminished emotional and mind-body scores.
Figure 1
FertiQoL subscale scores by gender and cause of infertility
Note. FertiQoL – fertility-related quality of life. Violin and box plots showing men’s and women’s scores on the (a) Emotional, (b) Mind-Body, (c) Relational, and (d) Social subscales of the FertiQoL questionnaire, categorized by the cause of infertility. Statistically significant differences between groups are indicated with p-values. FF – female factor; MF – male factor; MIX – mixed factor; UN – unexplained.
This result is consistent with previous literature demonstrating that more IVF treatment cycles correlate with a decline in the ability to cope emotionally with infertility and a more significant adverse effect on perceptions of daily physical and functional well-being (Celda-Belinchón et al., 2025; Ni et al., 2023). In our study, the effect on the Mind-Body scale was, notably, exclusive to women. This gender-specific outcome is likely a direct reflection of the cumulative physical burden of ART (Achilli & Pundir, 2021; Szalma, 2021). The cycle of hope and anxiety, combined with the invasive and demanding nature of the protocols, can directly impact a woman’s sense of well-being and integrity (Yu et al., 2021).
Our analysis also identified several sociodemo-graphic predictors. Individuals residing in mid-sized cities reported a higher quality of life. This aligns with general quality of life trends in the Czech Republic (Rypl et al., 2024) and likely reflects a confluence of factors relevant to the infertility experience, such as better access to specialized medical and psychological services, greater anonymity, which may reduce feelings of social stigma, and more diverse social networks outside of traditional family structures. Furthermore, higher household income was associated with better mind-body outcomes. While the cost of IVF in the Czech Republic is partially subsidized (Crouch, 2025), greater financial resources may provide a crucial “stress buffer.” This buffer could manifest as the ability to afford complementary therapies, take time off work for appointments without financial strain, or pursue other life-affirming goals (e.g., travel) that mitigate the all-consuming nature of infertility treatment (Gameiro & Finnigan, 2017). Of note, the couple’s financial standing and the size of the place of residence were two separate factors, as their association lacked practical significance (ρ = –.122, p = .010). Indeed, disposable household income in the Czech Republic is not associated with region or municipality size (Birčiaková et al., 2017).
Figure 2
FertiQoL subscale scores by gender and prior ART experience
Note. FertiQoL – fertility-related quality of life. Violin and box plots showing men’s and women’s scores on the (a) Emotional, (b) Mind-Body, (c) Relational, and (d) Social subscales of the FertiQoL, categorized by whether they have had prior assisted reproductive technology (ART) experience. A statistically significant difference between women with and without prior ART experience on the Mind-Body subscale is indicated with a p-value.
Interestingly, the life stage of the couple also appeared to influence outcomes. Being older was positively associated with Emotional and Mind-Body scores, perhaps a counter-intuitive finding given the age-related pressures of fertility (Chua et al., 2020; Igarashi et al., 2015; Shirasuna & Iwata, 2017). This may reflect greater emotional maturity, more established coping mechanisms, or having achieved other life goals that provide a more stable foundation from which to face infertility’s challenges (Livingstone & Isaacowitz, 2021; Pfund et al., 2024). With respect to relationship duration, the literature indicates that it has differential effects on men and women. Accordingly, our findings align with some previous studies while contradicting others. For example, Batool and de Visser (2014) found that for infertile women, a longer relationship duration was weakly (r = 0.2) associated with three negative outcomes: lower emotional satisfaction, lower perceived available support, and lower actually received support. On the other hand, García-Quintáns et al. (2023) reported that among men in infertile couples, a longer relationship duration was associated with better emotional adjustment. In our sample, longer relationship duration was negatively associated with Relational and Social scores. In other studies, no significant effect of partnership duration on relationship satisfaction was found (van Eickels et al., 2024). Hence, it can be inferred that relationship satisfaction is eroded more by the sustained accumulation of unresolved conflicts than by the simple passage of time in the partnership per se.
In an international context, the scores in our sample were broadly comparable to those from the German and Hungarian studies (Sexty et al., 2016; Szigeti et al., 2022), suggesting a shared experience of infertility in the broader region. However, nuanced differences, such as lower Social scores, may point to variation in cultural attitudes or the specifics of public discourse surrounding infertility in the Czech context.
Figure 3
FertiQoL subscale scores by gender and municipality size
Note. FertiQoL – fertility-related quality of life. Violin and box plots showing men’s and women’s scores on the (a) Emotional, (b) Mind-Body, (c) Relational, and (d) Social subscales of the FertiQoL, categorized by the population size of their municipality of residence. Statistically significant differences between groups are indicated with p-values.
However, the comparisons should be viewed with caution, since an important methodological consideration is that the data were collected in the period from July 2020 to February 2022, entirely within the global COVID-19 pandemic. This historical context represents a significant and unavoidable limitation, introducing a complex set of potential confounding variables that were not explicitly measured or controlled for in our research design. The pandemic precipitated a global health crisis that led to widespread, albeit transitory, disruptions in the provision of assisted reproductive technology (ART) services internationally (Chae-Kim et al., 2021; Chandi & Jain, 2021; Karaboue et al., 2022; Lam et al., 2022; Ory et al., 2020; Rallo et al., 2021). The initial guidance from major international regulatory bodies, such as the American Society for Reproductive Medicine (ASRM) and the European Society of Human Reproduction and Embryology (ESHRE) recommended the suspension of new, non-urgent treatment cycles to mitigate viral transmission and conserve healthcare resources (Veiga et al., 2020). These bodies also advised phased resumption of services with fundamentally altered operational protocols (ESHRE et al., 2020). The necessary modifications, including reduced patient capacity, staggered appointments, a significant shift to telehealth consultations, limitations on partners attending crucial appointments, and mandatory screenings – which were met with apprehension from patients (Marom Haham et al., 2021; Wedner-Ross et al., 2022) – not only limited service availability but also reshaped the patient experience in ways that could contribute to high levels of anxiety, depression, and a sense of unfairness (Barra et al., 2022; Boivin et al., 2020; Correa Rancel et al., 2023; Gordon & Balsom, 2020; Jaiswal et al., 2022; Kirubarajan et al., 2023; Lablanche et al., 2022; Lawson et al., 2021; Tippett, 2022; Tokgoz et al., 2022). Our study did not capture specific data on whether participants personally experienced treatment delays or postponements. Such unmeasured experiences could systematically influence quality of life. For instance, patients whose childbearing plans were delayed might report markedly different distress levels than those who were able to proceed (Dong et al., 2021; Matsushima et al., 2023). Beyond logistical disruptions, the pandemic acted as a powerful, chronic, and universal psychosocial stressor, which likely influenced the mental health of our participants in ways that could confound their reported fertility-related quality of life (Arora et al., 2022; Cénat et al., 2021; Salari et al., 2020; Xiong et al., 2020). Patients undergoing fertility treatment, which is a population already demonstrating elevated psychological vulnerability (Carson et al., 2021; Crespo & Bestard, 2016; Martins et al., 2016; Milazzo et al., 2016; Patel et al., 2018; Ribeiro Neto et al., 2025; Vaughan et al., 2020), reported heightened levels of anxiety, depression, hopelessness, and stress during this period (Qi et al., 2024; Rosielle et al., 2021; Wójtowicz et al., 2025). A further layer of psychological burden stemmed from medical and biological uncertainties. The indefinite postponement of treatment schedules may have amplified anxiety related to the age-dependent decline in reproductive potential (Gürtin et al., 2022). Concurrently, emerging information and fears regarding the potential direct effects of SARS-CoV-2 infection and vaccination on male and female reproductive health and pregnancy outcomes (Diaz et al., 2022; Madjunkov et al., 2020; Patel et al., 2021; Wang et al., 2023) introduced a significant degree of stress and decisional conflict (Flynn et al., 2021; Kern et al., 2023; Wedner-Ross et al., 2022) for this population. In our study, we did not collect data on participants’ COVID-19 infection history, their vaccination status, their personal risk perception, or their specific pandemic-related psychological burdens. To sum up, it is highly plausible that the universal, chronic stress of the COVID-19 pandemic (e.g., Knolle et al., 2021) influenced the baseline levels of psychological distress and life satisfaction across our entire sample. This influence was nonetheless likely not uniform, as the emotional response to the pandemic was shown to be more pronounced in women (García-Fernández et al., 2021). The impact of the pandemic on well-being may have induced a “floor effect” or a homogenization of variance in the dependent variable, potentially attenuating the associations with the sociodemographic and medical variables of interest. In other words, the pandemic’s pervasive influence may have become a dominant determinant of well-being, thereby overshadowing the more nuanced effects of the variables we sought to investigate. The generalizability of our findings to a non-pandemic context must therefore be approached with significant caution. While this study provides a unique snapshot of the experiences of Czech couples during this period, future longitudinal research – ideally incorporating data from pre-, during-, and post-pandemic periods – is necessary to disentangle the distinct psychological impact of infertility from the confounding effects of a major public health crisis.
Figure 4
FertiQoL subscale scores by gender and net household income
Note. FertiQoL – fertility-related quality of life. Violin and box plots showing men’s and women’s scores on the (a) Emotional, (b) Mind-Body, (c) Relational, and (d) Social subscales of the FertiQoL, categorized by net household income. Statistically significant differences between groups are indicated with p-values.
Another limitation of the present study is that we did not collect data on several potentially confounding health variables, such as participants’ general health status, comorbidities, or body mass index (BMI). The absence of this information prevents us from disentangling the psychological effects of infertility from the impacts of general physical health (Cao et al., 2023; Nagórska et al., 2022; Rodino et al., 2016; Wdowiak et al., 2021). We also did not gather detailed information on specific fertility treatment protocols, which vary in their physical and emotional demands (Blockeel et al., 2019; Coticchio et al., 2021; Santos-Ribeiro et al., 2019). Furthermore, to enhance procedural efficiency, the collection of select sociodemographic data was limited to a single partner; a parallel assessment from both would have enhanced data robustness and allowed for a more complex analysis of couple dynamics.
Finally, the FertiQoL instrument, while widely used internationally, has not yet been formally standardized for the Czech population. The rationale for its selection was its established utility in enabling cross-national comparisons with other European samples (Makara-Studzińska et al., 2022; Sexty et al., 2016; Szigeti et al., 2022; Warchol-Biedermann, 2021; Wdowiak et al., 2021). However, in comparison, our sample consisted primarily of couples in the initial stages of treatment. This composition may have led to an underestimation of the gender difference in QoL, as this gap might widen with the cumulative burden of prolonged and repeated treatment cycles. Future research is critically needed to address these limitations, ideally employing longitudinal designs that track couples from a pre-treatment, non-pandemic baseline through multiple ART cycles while collecting comprehensive health and dyadic data.
While our model identified key medical and sociodemographic predictors of fertility-related quality of life, it is a further limitation that we did not include a broader range of psychosocial variables. Future research would benefit significantly from incorporating measures of perceived social support, which is known to act as a critical buffer against distress in couples facing infertility (Abulizi et al., 2023; Casu et al., 2019; Kiesswetter et al., 2020; Shin et al., 2021). Similarly, assessing individual and dyadic infertility-related stress levels and coping strategies could provide a more dynamic picture of how couples navigate their situation (Andrei et al., 2021; Swift et al., 2021; Zurlo et al., 2018). Furthermore, exploring specific health beliefs, such as treatment optimism or perceived personal control, could help explain variations in well-being not captured by demographic or medical factors alone (Porat-Katz et al., 2016; Pugi et al., 2021; Schick et al., 2016; Zarbo et al., 2018). Integrating these psychological and social constructs would enhance the explanatory power of future models and allow for the development of more targeted clinical interventions.
Notwithstanding its limitations, the present study possesses a number of methodological strengths. A primary strength is the recruitment of a large, homogeneous sample of couples. The inclusion criteria specified couples experiencing primary infertility – defined as the woman having no prior pregnancies and the man having no biological children – a decision predicated on evidence suggesting that primary infertility is associated with more adverse outcomes across various domains than secondary infertility (Bernet et al., 2025; Dilbaz et al., 2012; Dural et al., 2016; Karabulut et al., 2013; Wadadekar et al., 2021). The diagnostic accuracy was ensured through recruitment by reproductive medicine specialists. A further significant strength lies in the application of the Actor-Partner Interdependence Model (APIM). This robust dyadic analysis technique, which is infrequently employed in infertility research, enabled an examination that transcended individual-level data to elucidate the interdependent nature of the couples’ experience. This approach is critical, as studies treating individuals as the unit of analysis fail to account for the non-independence of dyadic data, which can result in biased effect estimates.
CONCLUSIONS
In conclusion, this study’s dyadic approach provides a nuanced understanding of the interdependent experiences of couples facing primary infertility. Our findings confirm that gender is a primary determinant of fertility-related quality of life, while also revealing that the specific cause of infertility and prior treatment history create distinct points of vulnerability for both partners. We identified that women bear a disproportionate psychological burden, especially after previous ART attempts, and that men with a malefactor diagnosis represent a unique at-risk group.
The clinical implications of our findings are clear and actionable. They highlight the urgent need for integrated psychological support to be a standard component of fertility care. This support should be proactively offered to all patients, but with a particular focus on women, who consistently show higher vulnerability. Crucially, however, our results dismantle the notion that men are a monolithic group. Men with a male-factor diagnosis constitute a distinct high-risk population requiring targeted psychological intervention, perhaps through support groups or individual counseling that addresses feelings of shame and damaged identity. The disparities associated with municipality size also suggest that clinics should consider developing outreach or telehealth mental health programs to ensure equitable access for patients in underserved areas. By systematically monitoring patient well-being, clinicians can not only improve quality of life but can also significantly enhance treatment adherence and reduce premature dropout rates, as previously suggested, e.g., by Ghorbani (2022, 2025). Ultimately, a dyadic and context-sensitive approach is essential for providing equitable and effective care in reproductive medicine.