BACKGROUND
Perfectionism is a multidimensional trait of personality characterized by setting unrealistic standards, striving for flawlessness, and experiencing both external and internal pressures to be perfect (Frost et al., 1990). Perfectionism is frequently understood as a multidimensional personality trait with two higher-order dimensions termed perfectionistic concerns (PC) and perfectionistic strivings (PS) (Gäde et al., 2017), which can be extrapolated from the most widely used perfectionism measures (Stoeber, 2018). PC refers to extraordinarily critical appraisals of one’s own behavior, chronic harsh self-scrutiny, and excessive preoccupations with others’ evaluations, expectations, and criticism, while PS comprise the propensity to set excessively high personal standards that are often unrealistic in nature and to demand nothing less than perfection from the self (Sirois, 2016).
Previous research has suggested that perfectionism is one of the major personality factors that have an impact on health. Specifically, PC is consistently related to poorer health (Molnar et al., 2012a), greater psychopathology (Shafran & Mansell, 2001), and poorer well-being (Chang, 2000). On the other hand, PS is associated with both better and worse health. PS has been associated with higher levels of positive affect (Bieling et al., 2003), greater life satisfaction (Bergman et al., 2007), and better physical health (Molnar et al., 2006). However, it has also been detected as a risk factor for physical health (Fry & Debats, 2011), and in the last decades perfectionism has emerged as a personality trait construct that can also predict important health outcomes such as life-expectancy and mortality (Fry & Debats, 2009, 2011; Kozlowska & Kuty-Pachecka, 2023), emphasizing the importance of this construct in aging.
On the one hand, some studies have shown the impact of perfectionism on mental health in older adults (Chang, 2000; Karaminia et al., 2013). Karaminia et al. (2013) found that positive consequences of PS promote mental health of older people. However, Chang (2000) found that general perfectionistic tendencies were associated both directly and indirectly (through stress) with negative psychological outcomes (i.e. negative mood and worry). Furthermore, a large body of evidence has confirmed the association between perfectionism and psychological distress, including stress, anxiety, and depression (Flett et al., 2002; Hewitt et al., 2022).
On the other hand, only one study has studied the association between perfectionism and physical health in older adults more deeply. Molnar et al. (2012a) found that in older women with fibromyalgia PC was associated with poorer health functioning while PS had a non-linear relationship, such that exceptionally high and exceptionally low levels of PS were associated with poorer health functioning. Research on the relationship between perfectionism and physical health status in older adults is still scarce. Another gap in the literature is that much of the research on perfectionism and physical health has relied solely on self-report assessments of health outcomes.
In this aging scenario, objective fitness measures (a set of attributes related to a person’s ability to perform physical activities that require aerobic capacity, endurance, strength, or flexibility) have been shown to have a strong association with many and diverse health outcomes (Ortega et al., 2018). For instance, having moderate-to-high levels of muscular strength has been shown to be related to a lower risk of all-cause mortality and cancer mortality in older adults aged 60 years and over (McGrath et al., 2018). Cardiorespiratory fitness (CRF) is also a common predictor of the risk of mortality in this population (Sui et al., 2007). Moreover, balance disorders are among the most common causes of falls and negatively influence quality of life and survivorship with age (Cesari et al., 2009), so it might be considered among the objective fitness measures in older adults. Notwithstanding, there are no studies about these fitness outcomes and perfectionism among older adults despite the well-documented relationship between physical fitness and mental health in older adults (Navarra et al., 2023).
Moreover, the so-called psychological distress factors may be mediating this relationship. Depressive symptomatology has been associated with reduced levels of functioning in older adults (Garber et al., 2010), while increases in anxiety in late adulthood were associated with age-related losses in physical and cognitive functioning (Tetzner & Schuth, 2016). Psychological states play an integral role in the development and/or exacerbation of physical health issues and are key factors to consider for understanding how perfectionism might confer risk or benefit for physical health (Sirois & Molnar, 2016).
In this line, few studies have suggested that the relationship between perfectionism and health or physical health may be mediated by psychological outcomes such as affectivity, perceived stress, and perceived social support (Molnar et al., 2006, 2012a). Specifically, Molnar et al. (2012a) found that the association between PC and poorer health was mediated by higher levels of perceived stress and lower levels of perceived social support, while the association between PS and poorer health was mediated by higher levels of perceived stress and the association of PS and better health via higher levels of perceived social support. Similarly, Molnar et al. (2006) suggested that PS was associated with better physical health through high positive affect and low negative affect. In contrast, PC was associated with poorer physical health, and this relationship was partially mediated by low positive affect and high negative affect.
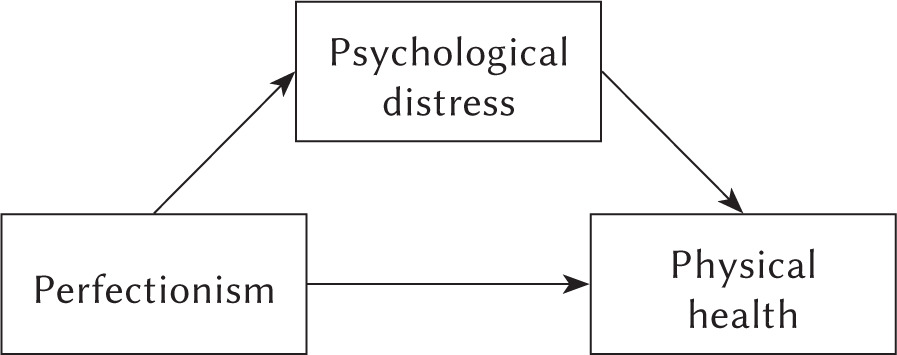
According to our knowledge, no studies have investigated whether the association between perfectionism and physical health (assessed through objective measures of fitness) is mediated by psychological state in older adults. The present study aimed to test the hypothesis that psychological distress mediates the relationship between perfectionism and physical health among older adults. Based on the previous literature, we hypothesized that PC would be associated with poorer health via higher levels of psychological distress, and PS would be associated with better physical fitness through lower levels of psychological distress.
PARTICIPANTS AND PROCEDURE
PARTICIPANTS
This single-centre, cross-sectional study included 131 older adults who were recruited through the University of Valencia and public healthcare facilities in Valencia, Spain (between September 2022 and September 2023). Recruitment was based on a medical derivation regarding the following criteria: Inclusion criteria comprised aged over 60 years and participation in a session of physical exercise. Exclusion criteria were a score < 24 points in the Mini Mental State Examination (Folstein et al., 1975) and the presence of any disorder that would prevent physical activity. Based on meeting these criteria, all participants received information from their primary care physician about their participation in a research programme and signed an informed consent form.
The study adopted a cross-sectional design with two days of data collection separated by about 48 hours. On the first day, participants completed the cognitive status questionnaire and underwent the upper limb strength test. On the second day, participants completed the questionnaires of perfectionism and psychological distress and were also evaluated for balance, and cardiorespiratory fitness. Ten individuals did not attend both days of assessments for reasons not related to the study; thus, 121 participants (71.50 ± 6.61 years; 90 women) were included in the statistical analyses. An a priori power analysis using G*Power (Faul et al., 2009) was conducted to determine the sample size needed to test the hypothesized model adequately. Assuming an effect size of f2 = 0.15, power set to 0.95 and α set to 0.05, the analysis revealed a required sample size of 119. Our sample of 121 participants was sufficient to detect effects.
All participants were informed both in writing and verbally about the experimental procedure and signed the written consent form of this study, which complies with the ethical standards of the Declaration of Helsinki 2013 and was approved by the ethics committee of the Hospital Clinico Universitario INCLIVA.
MEASURES
Perfectionistic concerns and perfectionistic strivings were assessed with two dimensions of the Spanish version of the Multidimensional Perfectionism Scale (MPS; Frost et al., 1990). The nine items of the “concern over mistakes” dimension were used as indicators of PC, and the seven items of the “personal standards” dimension were used as indicators of PS (Stoeber & Otto, 2006). The items were scored on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). By averaging items for each dimension, we created a media PC score (range 1-5), and a media PS score (range 1-5) that were used in the statistical analyses. Moreover, the total score of each dimension, by summing up the items, was used to describe the sample. Higher scores on these dimensions reflect greater levels of perfectionism. Cronbach’s alphas were .88 and .79 for perfectionistic concerns and strivings, respectively.
Psychological distress was measured through the Spanish version of the Depression, Anxiety, and Stress Scale-21 (DASS-21; Ruiz et al., 2017). It consists of 21 items with seven questions dedicated to each negative emotional state. The items are scored on a 4-point response scale with 0 – did not apply to me at all, 1 – applied to me to some degree/some of the time, 2 – applied to me to a considerable degree/a good part of time and 3 – applied to me very much/most of the time. By averaging items for each psychological state, we calculated the mean outcome (range 0-3), with higher scores indicating more severe depressive, anxiety, or stress symptoms. The total score of each dimension, by summing up the items, was used to describe the sample. Cronbach’s α for the depressive symptoms scale was .88, for anxiety was .82, and for stress was .88.
Cardiorespiratory fitness was assessed by means of the 200-meter walking test (200MWT) performed up and down in a corridor of 50 m as rapidly as possible, without running (Casillas et al., 2013). The mean gait speed in m/s was calculated and considered for the statistical analysis.
Balance was assessed by mini-BEST test in its Spanish version (http://www.bestest.us/test_copies). According to O’Hoski et al. (2015), the mini-BEST test assesses dynamic balance through 14 items that include four domains: anticipatory postural adjustments, postural responses, sensory orientation and stability in gait. Scores range from 0 to 2 for each item. The total score is 28 and higher scores indicate better balance. The total score of this test was used in the analysis (O’Hoski et al., 2015).
Upper limb strength was measured using the handgrip test (HG) with the Takei 5401 adaptive dynamometer (Takei Scientific Instruments Co., Ltd.), adjusted to each participant. Three measurements were taken on each arm with a one-minute rest, while maintaining the force for five seconds, and the mean value of the best score of both arms was taken for statistical analysis.
STATISTICAL ANALYSES
We performed the data analysis using SPSS v. 27 employing a statistical significance level of p < .05. Descriptive analyses were calculated to describe the sample characteristics. An a priori power analysis was conducted to determine the sample size needed to test the hypothesized model adequately, using an alpha error of 0.05, a power level of 0.80, and an RMSEA of at least 0.06, which corresponds to acceptable model fit (Hu & Bentler, 1999). This analysis was conducted with the semPower package in R. Concerning the hypothesized model (Figure 1), we tested the mediation model assessing psychological distress (i.e., depression, anxiety, and stress) as the mediator in the relationship between perfectionism and physical health, using the PROCESS macro with 5000 bootstrap samples and unstandardized regression coefficients. All the effects were evaluated through 95% bias-corrected confidence intervals (CIs). Effects were considered significant if their confidence intervals did not include zero.
RESULTS
Table 1 presents the characteristics of the participants. As established in the exclusion criteria, no subject with a Mini Mental State Examination score below 24 points participated in this study, so the cognitive status can be considered as “normal” (Monroe & Carter, 2012). Regarding cardiorespiratory fitness, all participants were able to walk above 0.9 m/s, the minimum speed to be considered independent and non-frail older adults (Castell et al., 2013). In fact, values of cardiorespiratory fitness and upper limb strength were above the 90-95 percentile for their mean age (Rio et al., 2022; Vianna et al., 2007), and levels of balance were in line with the average of other groups of healthy adults (Dominguez-Olivan et al., 2020). Participants also showed slightly higher than average scores for symptoms of depression, anxiety and stress (Henry & Crawford, 2005), as well as slightly lower levels of perfectionism (Ecija et al., 2021; Robinson et al., 2021). Specifically, levels of perfectionistic strivings were higher than perfectionistic concerns. Broadly, these data reflect a group of healthy older adults.
Table 1
Characteristics of participants
Importantly, sex comparisons showed no significant differences for any perfectionism or psychological distress outcome, or cognitive status. However, differences between men and women were found regarding fitness variables (cardiorespiratory, balance and upper limb strength).
Results of Pearson correlations are shown in Table 2. As expected, both PS and PC correlated positively with all psychological distress indicators (i.e. depression, anxiety, stress). Higher physical fitness (in cardiorespiratory, balance, upper limb strength) were significantly correlated with lower depressive symptom load. Moreover, higher levels of balance were significantly correlated with lower anxiety symptoms. No correlations were found between perfectionism dimensions and physical fitness variables.
Table 2
Pearson associations between key variables of study
Although we found no association between perfectionism and physical fitness, we proceeded to test the hypothesized model. Indeed, according to Hayes (2017) a variable X can exert an indirect effect on a variable Y through another variable M even in the absence of an association between X and Y. Therefore, to test whether psychological distress variables (i.e., depression, anxiety, and stress) could mediate the relation between perfectionism (PS and PC) and physical health (cardiorespiratory fitness, balance, and upper limb strength), mediation models were tested separately.
Regarding the direct effects, higher scores in PS and PC predicted higher symptoms of depression, anxiety, and stress (see Figures 2, 3, and 4). Among psychological distress variables, higher anxiety symptoms predicted lower balance (Figure 3), and high symptoms of depression predicted lower levels of upper limb strength (Figure 4). However, we did not find any direct association between psychological distress variables and cardiorespiratory fitness (Figure 2). Lastly, no direct effects were observed between perfectionism dimensions (PS and PC) and physical fitness.
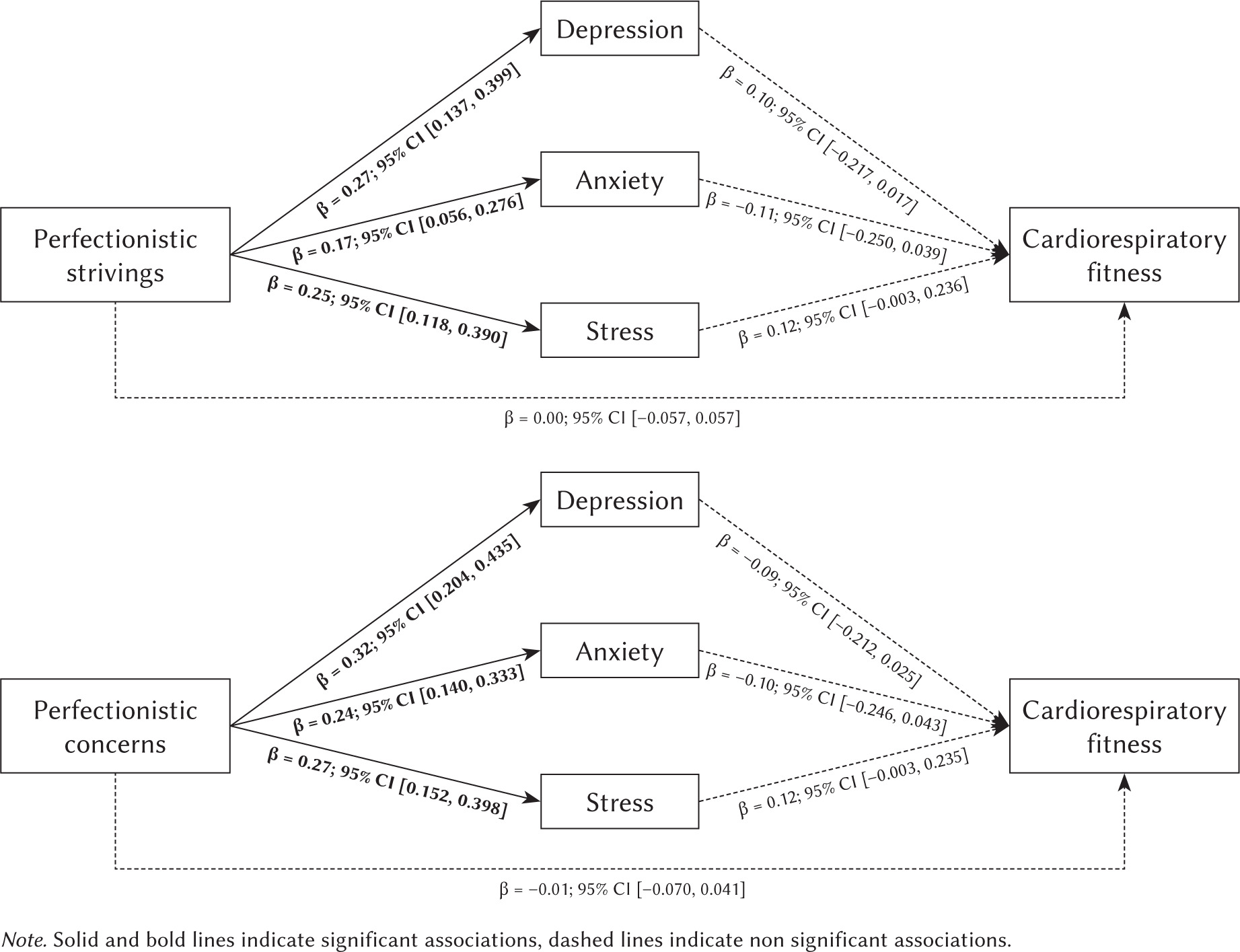
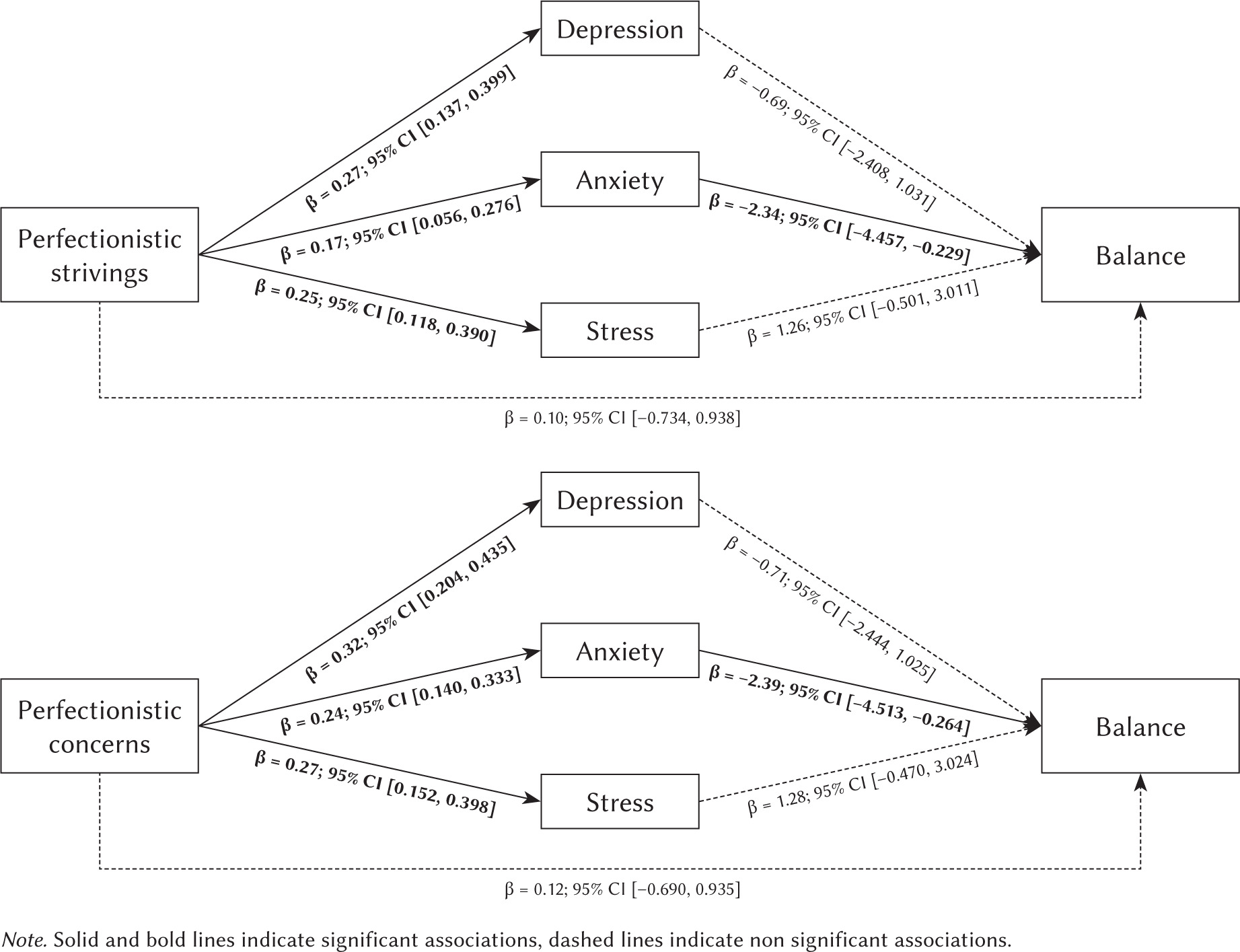
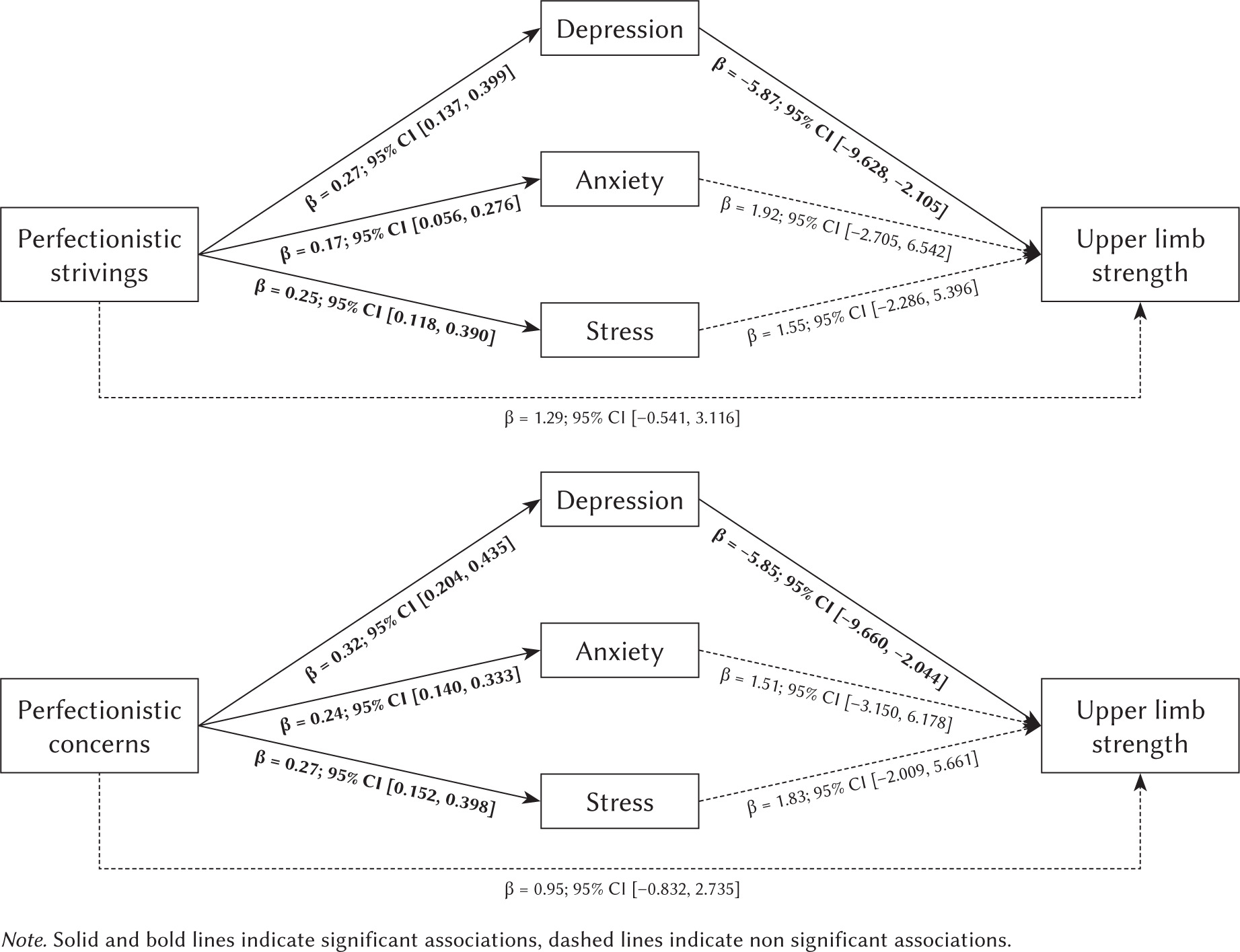
Table 3 reveals the findings of specific indirect effects of PS and PC on physical fitness of older adults (i.e. cardiorespiratory fitness, balance, and upper limb strength) through psychological distress (i.e. depression, anxiety, and stress). The indirect effects of PS and PC on balance through anxiety were –0.39 and –0.56, respectively (both p < .001). The indirect effects of PS and PC on upper limb strength through depression were –1.57 and –1.87, respectively (both p < .001). Hence, these results suggest that psychological distress mediates the relationship between perfectionism and older adults’ physical fitness.
Table 3
Results of indirect effects
Overall, PS and PC accounted respectively for 6.9% and 16.5% of the variance in anxiety, and for 7.6%, and 7.7% of the variance in balance. PS and PC accounted respectively for 12.1% and 20.1% of the variance in depression and for 9.0%, and 8.4% of the variance in upper limb strength. Interestingly, our results were confirmed when the hypothesized model was tested including sex as a covariate (further details can be requested from the authors).
DISCUSSION
Our results revealed that both PS and PC have an important effect on balance and upper limb strength through anxiety and depression, respectively. These findings contribute to the scarce current scientific literature about the association between perfectionism and physical health in older adults, adding new knowledge about the effect of personality and psychological distress in different objective physical fitness measures. Additionally, these findings have important public health implications, revealing a possible detrimental effect on physical health derived from perfectionism and poor mental health during aging.
On the one hand, our results showed that PS and PC were both positively linked with all psychological distress indicators in older adults (i.e. depression, anxiety, and stress). Our findings also indicate that PC is related more strongly to psychological distress than PS, confirming results previously reported in the literature (Burgess & DiBartolo, 2016). Broadly, PC has been consistently associated with negative psychological outcomes such as anxiety, depression, and stress in the general population (Chang, 2000; Juwono et al., 2023), considering PC as maladaptive perfectionism (Patterson et al., 2021). However, the evidence is controversial regarding PS. Whilst PS has been classified as adaptive or healthy perfectionism, since some authors have found that PS is often unrelated (or less related than PC) to anxiety and/or depression (Chang, 2017; Limburg et al., 2017), other researchers have discovered significant positive relationships between PS and psychological distress (Juwono et al., 2023; Smith et al., 2021). Therefore, our findings support the hypothesis that PS is not only associated with positive or adaptive correlates (Hill et al., 2018) in older adults. Unfortunately, the lack of similar studies in this population makes the comparison and interpretation of our results difficult.
On the other hand, regarding associations between psychological distress and physical fitness, there were no associations between stress and physical fitness outcomes, and a significant negative correlation between depression and CRF was lost when the entire model was tested. Notwithstanding, we found that higher levels of depression and anxiety were inversely associated with upper limb strength and balance, concurring with previous studies. For instance, Fábrega-Cuadros et al. (2020) found that greater anxiety levels were associated with poorer functional balance, which can be explained by a fear-of-fall related anxiety triggered by cognitive appraisals link to the vestibular loss during aging (Hull et al., 2013). Of importance, these same authors (Fábrega-Cuadros et al., 2020) did not find a relationship between psychological distress indicators and upper limb strength, opposite to us. Nevertheless, Smith et al. (2018) found that older adults with moderate to severe depressive symptoms had significantly lower handgrip strength scores than those with no or minimum depressive symptoms, especially among women and those who were obese. This suggests the importance of considering sex and weight status when investigating associations of this type. Even so, when we controlled for sex, the associations between depressive symptoms and upper limb strength were confirmed. In addition, the relationship between psychological distress and physical health in older adults seems to be bidirectional, since some studies have suggested that increasing functional disability is associated with greater the risk of suffering from psychological distress, and vice versa (Marques et al., 2021; Stegenga et al., 2012). In fact, improvements in physical function through exercise programmes can reduce psychological distress symptoms in older adults (Kazeminia et al., 2020). Our results highlight the importance of integrating physical, psychological, and social interventions to reduce or prevent psychological distress and low levels of fitness in older adults, dealing with well-being as a holistic construct that includes physical, social, and environmental components (Davitt et al., 2016).
One of the novelties of the present study rested on the hypothesis that perfectionism may exert its effects on older adults’ physical health via the intervening effects of psychological distress. Specifically, PS might be associated with better physical fitness through lower levels of psychological distress, and PC might be associated with poorer physical health via higher levels of psychological distress. Our findings supported only partially these hypotheses, since both PC and PS were associated with poorer physical health via higher psychological distress. Moreover, although no direct relationships were found for PS and PC with physical health variables, the estimation of significant indirect effects sustained the hypothesis that anxiety and depression partly mediated the effects that both PS and PC had on balance and upper limb strength, respectively. These findings are in line with Molnar et al. (2012b), who found that PC and PS were negatively associated with self-reported physical health via perceived stress in undergraduate students. By contrast, Molnar et al. (2006) found that PS was associated with higher levels of positive affect and lower levels of negative affect, which, in turn, were related to better health. These results highlight the importance of conducting further research in this field and might reflect a different pattern of association between perfectionism and physical health in students and older people. In this regard and to the best of our knowledge, the present study represents the first empirical effort providing evidence for a possible explanation for the association between perfectionism and objective measures of physical health in older adults. Finally, these findings clearly support the notion that psychological distress has an important role not only in the association between perfectionism and mental health but also between perfectionism and physical health (Besharat et al., 2011; Molnar et al., 2012b), at least in older adults.
This study has several implications for individual and public health, such as the importance of considering psychological factors when assessing and addressing fall risk and declining physical functioning in older adults. Furthermore, the findings suggest that learning healthy coping strategies to manage perfectionism and improve mental health could have direct benefits for preserving physical function as people age. This could include cognitive-behavioural therapies, workshops, or educational materials that promote healthy coping strategies, or seeking psychological support when needed.
The strengths of this study include an adequate sample size, and the use of objective physical health measures in older adults. Thereby, although subjective self-report measures of health have been shown to have good construct and predictive validity, objective measures can help to clarify the nature of the relationships of PS and PC with physical health, which may go beyond self-reported perceptions (Molnar & Sirois, 2016). However, this study has some limitations that should be mentioned. First, the sampling method and inclusion criteria might have created a risk of bias because the examined participants wanted to participate in a session of physical exercise. In addition, the cross-sectional design of our analyses prevents us from interfering causal relationships. Likewise, recent studies have shown that some variables, such as body mass index, can be important when analysing psychological distress or perfectionism (Rawat & Blachnio, 2025; Smith et al., 2018), so future studies should consider such covariates in the analyses. Lastly, there are numerous physical health variables that can be used to assess physical health in older adults. Future studies should explore this field of knowledge more deeply, testing other models and study variables to shed more light on the subject.
In conclusion, our results suggest that the associations between perfectionistic dimensions and upper limb strength and balance were mediated by depression and anxiety. From these findings, perfectionist older adults might benefit substantially from exercise training programmes, since physical exercise can improve both mental health and physical fitness, as well as other interventions designed to yield improvements in their social networks. This study adds to the growing literature illustrating the predictive utility of perfectionism in health. We are still in the beginning stages of understanding how perfectionism might benefit physical health in the long term. Succeeding in filling this knowledge gap can contribute to the promotion of mental and physical health of older adults globally and thus achieve some Sustainable Development Goals (SDGs), such as good health and well-being (SDG 3), or reduced inequalities (SDG 10).