BACKGROUND
Transgender is an umbrella term encompassing individuals whose gender identity or expression differs from the sex assigned to them at birth, or who identify with a gender different from their assigned sex (Kota et al., 2020). Globally, transgender people face many challenges in their daily lives, including discrimination, violence, and stigma due to their minority status in a heteronormative world (Cortes, 2017; Drabish & Theeke, 2022; European Union Agency for Fundamental Rights, 2014). Although notable progress has been made in securing rights for broader LGBT communities, transgender rights remain under-realized, and transgender individuals continue to experience restricted access to adequate housing, education, employment, and healthcare (James et al., 2016; Stocks, 2015; White Hughto et al., 2015). In many countries, particularly where transgender rights receive little legal recognition or protection, transgender individuals encounter considerable barriers to accessing genderaffirming interventions, which have been shown to help them overcome the gender-related stressors (Abreu et al., 2022; Huit et al., 2024; Tomita et al., 2019). Furthermore, the transgender populations are at an elevated risk of experiencing a range of mental health challenges, including depression, anxiety, and self-harm compared to non-transgender populations (Pinna et al., 2022; Rosenstreich, 2013; Su et al., 2016).
GENDER DYSPHORIA: DEFINITION AND PREVALENCE
Gender dysphoria, characterized as distress or discomfort resulting from the incongruence between the sex assigned at birth and gender identity, is a mental health issue uniquely experienced by transgender individuals (Byne et al., 2018). According to Cooper et al. (2020), this phenomenon is nuanced and may manifest in four different themes: (a) distress arising from the dissonance between assigned sex and experienced gender (e.g., shame about erections in transgender women); (b) the interface of assigned sex, gender identity, and societal expectations (e.g., disappointment and suicidal ideation when misgendered); (c) social consequences of gender identity (e.g., a diminished sense of belonging); (d) internal processing of rejection and transphobia (e.g., self-stigma and self-hatred due to internalized prejudices against transgender people). Gender dysphoria is diagnosed as a psychiatric condition when it significantly impairs functioning in transgender individuals (American Psychiatric Association, 2013).
Although the experience of gender dysphoria varies across regions and cultures, it may be experienced by transgender individuals of all ages and gender identities (American Psychiatric Association, 2013). A growing body of literature has shown that gender dysphoria is becoming increasingly prevalent among transgender populations (Jarvis et al., 2025; Wiepjes et al., 2018). For example, in the United States, the proportion of Americans aged 6 to 21 who experienced gender dysphoria rose nearly threefold, from 0.161% in 2016 to 0.475% in 2019 (Mitchell et al., 2022). Further, the number of transgender people attending gender identity clinics to seek help with their gender dysphoria has increased over time (Aitken et al., 2015; Wiepjes et al., 2018). Meanwhile, the average age of individuals experiencing gender dysphoria is decreasing, with prevalence peaking in the late teenage years and early twenties (Sun et al., 2023). While gender dysphoria has often been studied among binary transgender individuals (those who identify as either male or female), it is also present among nonbinary individuals, who identify as neither male nor female (Galupo et al., 2021; Lindley & Galupo, 2020; Silva et al., 2021). However, the experience of the latter group remains under-documented, as their gender dysphoria is often related to the difficulty of achieving an androgynous or fluid body ideal – an experience that differs significantly from traditional binary conceptualizations of gender dysphoria (Galupo et al., 2021). This highlights the need for more research that is inclusive of this group.
GENDER DYSPHORIA, PSYCHOLOGICAL DISTRESS, AND RESILIENCE
Research has shown that transgender individuals with gender dysphoria are more likely to experience psychological distress (Arvind et al., 2021; Davey et al., 2014). Compared to transgender individuals without gender dysphoria, those diagnosed with this condition report higher levels of psychological distress (Davey et al., 2014; Hilton et al., 2022). On the one hand, gender dysphoria can serve as a source of psychological distress, as individuals experiencing gender incongruence are frequently exposed to persistent gender-related discrimination and rejection, which are associated with elevated levels of depression and anxiety (Bechard et al., 2017; Lloyd et al., 2019). Mislabeling and stigmatization due to gender minority status may further exacerbate psychological distress (Cooper et al., 2020). On the other hand, psychological distress may predict symptoms of gender dysphoria by reducing self-acceptance and heightening sensitivity to bodily incongruence (Hilton et al., 2022; Mirabella et al., 2020).
In the face of gender-related adversity, resilience – the ability to adapt effectively to difficulties and challenges – can help transgender individuals achieve a more balanced life (VandenBos, 2015). Several factors have been identified as enhancing resilience among transgender people, including parental connectedness, social support, being addressed by one’s preferred name, safety and sense of belonging at school (Tankersley et al., 2021). Transgender individuals with gender dysphoria who are highly resilient tend to experience less stress, report greater life satisfaction, and receive more social support (Başar & Öz, 2016). Moreover, peer support, as a component of resilience, may buffer the relationship between stigma and psychological distress (Bockting et al., 2013). Having a positive role model can also help transgender people mitigate psychological distress and strengthen resilience (Matsuno & Israel, 2018). Conversely, low resilience is associated with increased psychological distress. For instance, transgender individuals who receive limited family support report lower levels of resilience and higher levels of psychological distress (Fuller & Riggs, 2018).
THE EXPERIENCE OF TRANSGENDER INDIVIDUALS IN VIETNAM
It is estimated that approximately 300,000 transgender individuals in Vietnam face numerous challenges in both legal and social contexts (Nguyen et al., 2025; Pham et al., 2018). Although the 2015 Civil Code introduced the possibility of gender identity reconfirmation and gender transition, the absence of guiding regulations and the delayed passage of the Gender Affirmation Law have rendered this provision unenforceable, leaving transgender rights unrecognized for years (Buchhave et al., 2023). In everyday life, transgender individuals in Vietnam are subjected to stigma and various forms of gender-based discrimination, including sexual harassment, as well as physical and verbal violence (Nguyen et al., 2025). Within the workplace, many report that such experiences, combined with limited educational attainment and the absence of anti-discrimination policies, hamper their opportunities for employment, promotions, benefits, and equal pay (Oosterhoff & Hoang, 2018). Even within their families, transgender individuals may be devalued for not fulfilling normative expectations of having biological children to continue the family lineage (Nguyen et al., 2025). These layers of stigmatization and marginalization are rooted in traditional cultural values strongly shaped by Confucian norms of rigid gender roles and binary classification (Grosse, 2015). Consequently, transgender people are often regarded as deviating from societal norms, and thus face widespread rejection and exclusion.
Previous studies indicate that a large proportion of transgender individuals in Vietnam experience gender dysphoria, described as profound discomfort with one’s body and feelings of disgust or fear when confronted with body parts associated with one’s biological sex (Ha, 2019; Pham et al., 2018). Gender dysphoria frequently emerges as a central theme of psychological distress among transgender individuals and may be further exacerbated by the lack of social recognition and inclusion (Hoang et al., 2024; Nguyen et al., 2025). Nevertheless, the relationship between gender dysphoria and other psychological constructs remains underexplored, as transgender mental health has received limited scholarly attention in Vietnam. Moreover, despite the evident needs resulting from gender incongruence, access to gender-affirming interventions and psychotherapy remains highly restricted, as many healthcare professionals lack adequate training to support transgender patients (Do & Nguyen, 2020). Some studies also show that transgender individuals, particularly transgender women, encounter significant financial and systemic barriers to health care, leading some to rely on non-medically prescribed hormone use, silicone injections, or sex reassignment surgery (Do et al., 2018; Nguyen, 2019). Taken together, these gaps in knowledge and contextual challenges underscore the urgent need for more research addressing the wellbeing of the transgender population in Vietnam.
PRESENT STUDY
In this study, we investigated the relationship between gender dysphoria and psychological distress among Vietnamese transgender individuals, with particular attention to the moderating role of resilience. Although resilience has been consistently shown to buffer the adverse effects of stressors on mental health (Başar & Öz, 2016; Singh et al., 2014), its role in the specific context of gender dysphoria has not been tested in previous research. Previous studies in Vietnam have documented experiences of gender dysphoria and related psychological difficulties, such as depression, sadness, disgust, frustration, and self-hatred among transgender individuals (Ha, 2019; Nguyen et al., 2025; Pham et al., 2018). However, these studies did not statistically examine the interrelationships among these variables, as they primarily relied on qualitative designs. Another limitation of the research to date is its exclusive focus on binary transgender individuals. Therefore, the present study adopted a more comprehensive approach by including nonbinary participants and aimed to highlight the need for enhanced mental health support for this community.
This study is grounded in Meyer’s (2003) Minority Stress Model, which posits that sexual and gender minorities are exposed to both distal stressors (e.g., discrimination) and proximal stressors (e.g., internalized stigma, gender dysphoria). Collectively, these stressors contribute to a wide range of detrimental mental health outcomes (Hendricks & Testa, 2012; Lindley & Galupo, 2020). Within this framework, resilience functions as a protective factor that buffers against the negative effects of such stressors (Testa et al., 2015). Applying this model, we conceptualized gender dysphoria as a proximal stressor, psychological distress as the outcome, and resilience as a moderator that may attenuate the adverse impact of gender dysphoria on psychological distress. Thus, the following hypotheses were proposed:
H1: Levels of gender dysphoria and psychological distress vary according to the sociodemographic characteristics of transgender individuals.
H2: Gender dysphoria is positively associated with psychological distress among transgender individuals.
H3: Resilience moderates the relationship between gender dysphoria and psychological distress.
PARTICIPANTS AND PROCEDURE
STUDY DESIGN AND PARTICIPANTS
The current study employed a cross-sectional design and used a combination of convenience and snowball sampling methods. The survey was created and administered via Google Forms, allowing participants to self-report anonymously. Vietnamese transgender individuals were recruited through an online link distributed via transgender groups on various social media platforms – primarily Facebook – as well as through intermediaries who were acquaintances of the research team. Upon accessing the survey link, participants were provided with information about the study’s objectives, eligibility criteria, confidentiality principles, and the voluntary nature of their participation. Those who consented to participate proceeded to answer demographic questions followed by measurement scales. Completing the survey took approximately 20 minutes. Upon completion, participants were encouraged to share the survey link with other members of the transgender community. Ethics approval for this study was granted by the Ethics Committee of the University of Social Sciences and Humanities, Vietnam National University, Hanoi.
The sample size for testing the moderation model was determined with a prior power analysis conducted using G*Power (Faul et al., 2009). Assuming a small-to-moderate effect size (f2 = .03), a significance level (p = .05), a desired statistical power of .80, one tested predictor, and three predictors in the model, the analysis indicated that a minimum of 264 participants would be required. The inclusion criteria for this study were: (1) being 16 years of age or older, (2) having Vietnamese as a native language, and (3) providing informed consent to participate in the study. The exclusion criteria included: (1) having a gender identity that matches sex assigned at birth, (2) omitting all items from at least one measurement scale, and (3) exhibiting signs of careless responding (e.g., selecting the same response option for all items).
A total of 570 individuals were approached, of whom 569 consented to participate and completed the survey, yielding a response rate of 99.8%. However, 222 responses were excluded, including 165 responses from individuals reporting congruence between their sex assigned at birth and their gender identity, and 57 responses that contained inconsistent answers to certain questions (e.g., income, gender identity disclosure). Ultimately, 347 valid responses were retained for analysis, with participants aged 16 to 44 (M = 23.87, SD = 5.1). Detailed information on the sociodemographic characteristics of the sample is presented in Table 1.
MEASURES
Data were collected on seven sociodemographic variables: (1) age, (2) sex assigned at birth (male or female), (3) gender identity (male, female, or neither), (4) sexual orientation (heterosexual, homosexual, bisexual, or other), (5) monthly income (having income or not), (6) relationship status (single or not), and (7) education level (high school or below, undergraduate, or postgraduate). Based on participants’ self-reported gender identity, they were categorized into three groups: transgender men, transgender women, and nonbinary individuals. In addition, participants were asked three questions regarding whether they had ever (1) considered and/or undergone gender-affirming interventions (e.g., hormone replacement therapy or gender-affirming surgery), (2) disclosed their gender identity (i.e., come out) to at least one person, and (3) participated in transgender support groups.
Utrecht Gender Dysphoria Scale – Gender Spectrum (UGDS-GS; McGuire et al., 2020) was used to measure gender dysphoria. It consists of 18 items assessing both desire to live in accordance with one’s gender identity (e.g., “I always want to be treated like my affirmed gender”) and distress related to one’s assigned sex (e.g., “Every time someone treats me like my assigned sex, I feel hurt”). Participants were asked to indicate the extent to which they agreed with each item on a 5-point Likert scale ranging from 1 (disagree completely) to 5 (agree completely). The total score of the UGDS-GS ranges from 18 to 90, with higher scores indicating greater levels of gender dysphoria. As no official Vietnamese version of the UGDS-GS was available, the scale was translated from English into Vietnamese and subsequently revised by members of the research team. In the present study, the UGDS-GS demonstrated excellent internal consistency (Cronbach’s α = .95).
Kessler Psychological Distress Scale (K10; Kessler et al., 2003) with a Vietnamese version translated by Pham (2015) was employed to evaluate psychological distress. The K10 comprises 10 items that measure emotional distress experienced over the past 30 days (e.g., “During the last 30 days, about how often did you feel hopeless?”). Responses are rated on a 5-point Likert scale ranging from 1 (none of the time) to 5 (all of the time). Total scores range from 10 to 50, with higher scores reflecting greater levels of psychological distress. In the present study, the K10 demonstrated high internal consistency (Cronbach’s α = .94).
Connor-Davidson Resilience Scale (CD-RISC-10; Campbell-Sills & Stein, 2007) adapted for the Vietnamese population by Minh-Uyen and Im (2020) was used to measure resilience over the past month. This scale assesses an individual’s ability to adapt to changes and overcome life challenges (e.g., “I can deal with whatever comes”). Responses are collected based on a 5-point Likert scale ranging from 0 (strongly disagree) to 4 (strongly agree). Total scores range from 0 to 40, with higher scores indicating greater levels of resilience. In the present study, the CD-RISC-10 showed robust internal consistency (Cronbach’s α = .94).
STATISTICAL ANALYSIS
Due to missing data, missing values on continuous variables were imputed using the mean of each respective variable. Missing values on categorical variables (i.e., demographic variables) were retained as they were. To test the proposed hypotheses, we conducted descriptive statistics, mean comparison analyses (independent t-tests and one-way ANOVA with Bonferroni post hoc test), and Pearson correlation analyses using SPSS version 26.0. The moderating role of resilience in the relationship between gender dysphoria and psychological distress was tested using Model 1 of the PROCESS macro (version 4.2; Hayes, 2018). The analysis employed 5,000 bootstrap resamples with 95% bias-corrected confidence intervals (CIs). A bootstrap CI that did not include zero was interpreted as evidence of a statistically significant moderating effect. Prior to conducting the moderation analysis, the statistical assumptions for regression with an interaction term (gender dysphoria × resilience) were assessed. The model met the assumptions of linearity, normality of residuals, independence of errors, absence of multicollinearity, and homoscedasticity.
All analyses employed two-tailed tests, and statistical significance was determined using an alpha level of .05. Effect size indices used in the analyses included Cohen’s d for independent t-tests, Cohen’s f for oneway ANOVA, Pearson’s r for correlation analyses, and Cohen’s f2 for regression analyses involving interaction terms (moderation analysis). The cut-off values for small, medium, and large effect sizes followed the guidelines proposed by Cohen (1988). Effect size estimation and sensitivity power analysis were performed using G*Power software (Faul et al., 2009).
Table 1
Sociodemographic characteristics of the sample (N = 347)
[i] Note.aAccording to the General Statistics Office of Vietnam (2023), the average monthly income of workers in 2023 was VND 7.1 million. We used VND 7 million as the cut-off point.
RESULTS
GENDER DYSPHORIA AND PSYCHOLOGICAL DISTRESS LEVELS AMONG TRANSGENDER PEOPLE
The mean total score of UGDS-GS for the whole sample was 64.96 (SD = 16.1), ranging from 18 to 90. Variations in the level of gender dysphoria were observed based on several sociodemographic characteristics. Transgender individuals who were younger, identified as nonbinary, had a bisexual orientation, and reported no intention of undergoing gender-affirming interventions (e.g., surgery or hormone therapy) reported lower levels of gender dysphoria. In contrast, participants with above-average income (VND 7 million or more), those who had disclosed their gender identity, and those who had participated in transgender support groups experienced higher levels of gender dysphoria. No significant differences in gender dysphoria were found based on sex assigned at birth or educational attainment.
Regarding psychological distress, the total K10 score had a mean of 25.50 (SD = 8.9), with values ranging from 10 to 50. Overall, levels of psychological distress were relatively consistent across sociodemographic groups. Notably, participants who had not yet undergone any gender-affirming interventions but intended to do so in the future reported higher levels of psychological distress compared to those who had partially undergone such interventions. Furthermore, individuals who had not disclosed their transgender identity experienced greater psychological distress than those who had come out.
For statistically significant group comparisons, most effect sizes ranged from small to moderate (Cohen’s d ranged from 0.29 to 0.55; Cohen’s f ranged from 0.19 to 0.34). An exception was observed in the difference in gender dysphoria based on participation in transgender support groups, which yielded a large effect size (d = 1.76). Detailed results are shown in Table 2.
Table 2
Comparison of gender dysphoria and psychological distress level among participants
RELATIONSHIP BETWEEN GENDER DYSPHORIA, PSYCHOLOGICAL DISTRESS, AND RESILIENCE
The results of the correlation analysis among the variables are presented in Table 3. The association between gender dysphoria and psychological distress was positive and of small size (r = .16, p = .002). In contrast, resilience was negatively correlated with psychological distress (r = –.16, p = .004).
Table 3
Pearson correlation coefficients between studied variables
| 1 | 2 | 3 | |
|---|---|---|---|
| 1. Gender dysphoria | – | ||
| 2. Psychological distress | .16** | – | |
| 3. Resilience | .42*** | –.16** | – |
Table 4
Moderation analysis of the role of resilience in the relationship between gender dysphoria and psychological distress
| B | SE | t | LLCI | ULCI | R2 | F | |
|---|---|---|---|---|---|---|---|
| Gender dysphoria | .15 | .03 | 4.82*** | .089 | .211 | .11 | 14.09*** |
| Resilience | –.26 | .05 | –4.89*** | –.369 | –.157 | ||
| Gender dysphoria × Resilience | –.01 | .00 | –2.95** | –.013 | –.003 |
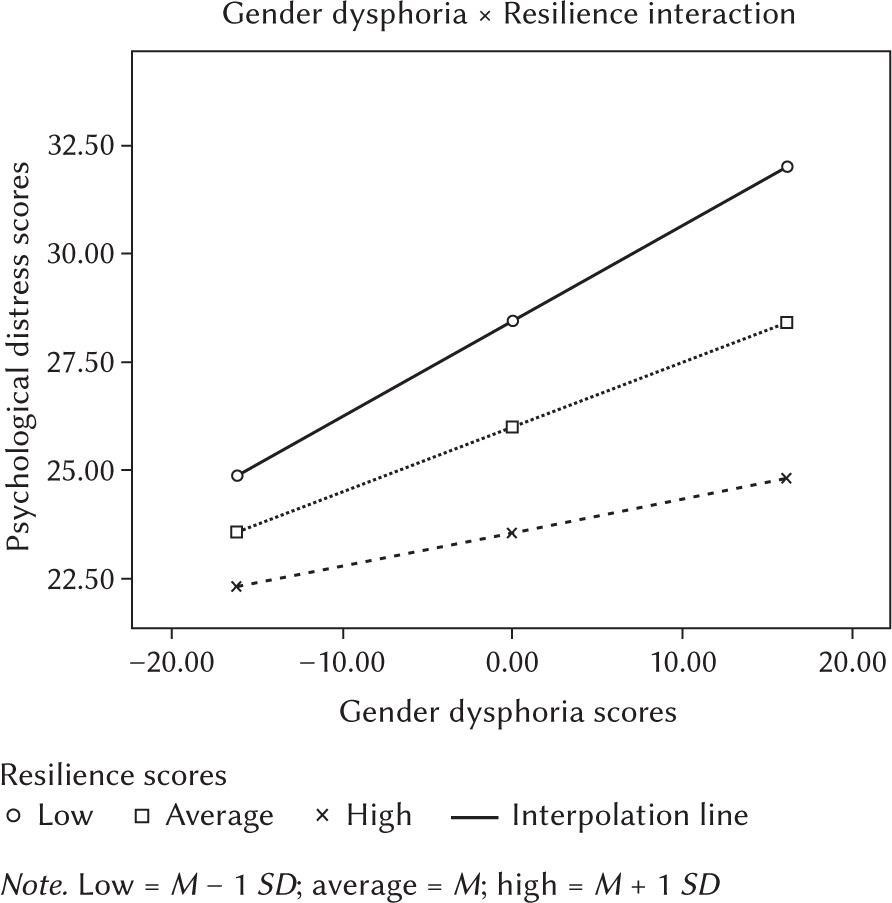
The moderation analysis (see Table 4) revealed that 11.0% of the variance in psychological distress was explained by gender dysphoria, resilience, and their interaction. The interaction term between gender dysphoria and resilience was statistically significant (∆R2 = 2.3%, f2 = 0.02, p = .003), indicating a small but meaningful moderating effect of resilience on the relationship between gender dysphoria and psychological distress. A simple slopes analysis was conducted to further examine this interaction. The results showed that gender dysphoria was positively associated with psychological distress among participants with low levels of resilience (B = .22, SE = .04, 95% CI [.146, .298], p < .001) and moderate levels of resilience (B = .15, SE = .03, 95% CI [.089, .211], p < .001). However, the association was not statistically significant among participants with high levels of resilience (B = .08, SE = .04, 95% CI [–.002, .157], p = .054 [see Figure 1]).
DISCUSSION
LEVELS OF GENDER DYSPHORIA AND PSYCHOLOGICAL DISTRESS AMONG TRANSGENDER INDIVIDUALS
The results showed that there were certain differences in levels of gender dysphoria and psychological distress across sociodemographic groups (H1 partially supported). Regarding gender dysphoria, the mean UGDS-GS score in the overall sample (M = 64.96) was lower than the score observed in a Thai sample (M = 77.82; Jamneankal et al., 2023), but higher than that of a Chinese sample (M = 49.52; Li et al., 2024). These variations may reflect differences in sociocultural context or characteristics of the studied samples. Nevertheless, the findings underscore that gender dysphoria remains a significant psychological concern among Vietnamese transgender individuals, consistent with evidence from both quantitative and qualitative studies (Nguyen et al., 2025; Pham et al., 2018). In contemporary Vietnamese society, the lack of specialized healthcare services for transgender people and systemic discrimination have significantly limited this community’s access to gender-affirming interventions (Do & Nguyen, 2020; Do et al., 2018; Nguyen et al., 2025). These difficulties may not only exacerbate gender-related distress but also hinder efforts to address it. Additionally, the current study found that transgender individuals who were older, identified with a binary gender identity, and reported a heterosexual sexual orientation experienced higher levels of gender dysphoria. These findings stand in contrast to previous research (Chen et al., 2023; Li & Zheng, 2023; Murawsky, 2023; Oshima et al., 2022). For instance, Schneider et al. (2016) suggested that older individuals, who typically experience earlier onset of gender dysphoria, tend to develop more coping strategies to manage gender-related distress over time. It was also unexpected that nonbinary transgender individuals reported lower levels of gender dysphoria, as they are known to face more prejudice and pressure to conform to strict binary trans-normativity (Lindley & Galupo, 2020; Murawsky, 2023; Osborn, 2022). In terms of sexual orientation, bisexual participants reported lower levels of gender dysphoria compared to heterosexual participants, which is contrary to the idea that non-heterosexual transgender individuals may experience greater distress due to societal expectations around gender roles (Chen et al., 2023). Therefore, these findings should be interpreted with caution, particularly given the relatively small effect sizes observed. Other factors such as intending to undergo gender-affirming interventions, being in a relationship, having come out, and being involved in a transgender community were associated with higher risk of gender dysphoria. Those with higher levels of gender dysphoria were more likely to seek gender-affirming treatment because it could help reduce body dissatisfaction and enhance well-being (Foster Skewis et al., 2021; van Leerdam et al., 2023). Many transgender people may also tend to seek support from family, peer groups, and romantic partners by coming out to them (Li & Zheng, 2023). However, dating and interacting in interpersonal relationships may increase the risk of transgender people being exposed to potential external factors that trigger gender dysphoria (Galupo et al., 2020).
With respect to psychological distress, the mean K10 score in the current study (M = 25.50) was lower than that reported in transgender samples from Pakistan (M = 34.16; Falak et al., 2020) and North America (M = 28.70; Fuller & Riggs, 2018). However, this finding still indicates a high level of psychological distress among Vietnamese transgender individuals, falling within the moderate-to-severe range (22-29) based on the thresholds proposed by Slade et al. (2011). This result underscores the mental health risks associated with chronic exposure to violence and discrimination within both familial and broader social contexts (Nguyen et al., 2025). Moreover, consistent with previous research, the present study found that psychological distress was elevated among individuals who had not disclosed their gender identity or who experienced delays in accessing gender-affirming interventions (Fontanari et al., 2020; Rood et al., 2017).
ASSOCIATION BETWEEN GENDER DYSPHORIA AND PSYCHOLOGICAL DISTRESS
An important finding of the present study is that gender dysphoria was positively correlated with psychological distress among transgender individuals (H2 substantiated). Consistent with previous studies, this result reinforces the understanding that gender dysphoria is a significant risk factor for mental health concerns in transgender populations, including general psychological distress (Austin et al., 2022; Pease et al., 2023) as well as specific issues such as depression, anxiety, and suicidality (Brokjøb & Cornelissen, 2022; Li & Zheng, 2023; Li et al., 2024). This finding also aligns with the view that gender dysphoria represents one of the most central proximal stressors faced by the transgender community in the Minority Stress Model (Cao et al., 2024; Meyer, 2003). Conceptualizing gender dysphoria as a stressor – rather than a pathological mental health condition – shifts the focus from individual psychopathology to the sociocultural pressures experienced by transgender individuals (Galupo et al., 2020; Lindley & Galupo, 2020). Importantly, gender-related distress is not derived solely from gender incongruence itself, but also from the stigma embedded in cis-normative social structures (Bouman et al., 2010). In a qualitative study by Galupo et al. (2020), participants described this form of distress as intrusive thoughts and persistent concerns about how others read and think about their gender. Thus, gender dysphoria may also be understood as a process of internalizing and self-enforcing rigid gender norms, thereby causing distress due to feelings of alienation and rejection (Pease et al., 2023).
MODERATING ROLE OF RESILIENCE
The most novel finding of the present study is that resilience moderated the relationship between gender dysphoria and psychological distress (H3 substantiated). To the authors’ knowledge, no prior research has investigated the moderating role of resilience in the relationship between gender dysphoria and mental health outcomes. Nonetheless, a growing body of literature suggests that resilience, at both the individual and community levels, serves as a protective factor against the mental health risks faced by individuals with gender dysphoria (Başar & Öz, 2016; Scandurra et al., 2017; Singh et al., 2014). In line with the Minority Stress Model, psychological resilience has been shown to buffer detrimental effects of various stressors, including gender-based discrimination (Scandurra et al., 2017; Zhang et al., 2021) and horizontal internalized transphobia (i.e., alienation from the transgender community; Scandurra et al., 2018). Therefore, the current finding further extends this perspective by demonstrating that resilience also mitigates the psychological burden of gender dysphoria. Under challenging circumstances, resilience enables transgender individuals to navigate stress effectively by fostering adaptability and facilitating the mobilization of internal resources (Catelan et al., 2022; Zimmerman, 2013). Consequently, resilience may help alleviate the psychological distress associated with gender dysphoria and promote solution-focused coping strategies. Moreover, resilience among transgender people can manifest in various forms, such as pride in one’s identity, a sense of community connectedness, and access to social support (Puckett et al., 2024a). While the current study focused on individual-level resilience, future research is encouraged to explore additional dimensions of resilience, including relational and group-level aspects.
PRACTICAL IMPLICATIONS AND LIMITATIONS
The present study provides empirical evidence of the detrimental impact of gender dysphoria on the mental health of Vietnamese transgender individuals and highlights the potential protective role of resilience against this effect. Based on these findings, several implications may be considered for policymakers and healthcare providers. Recognizing gender dysphoria as a proximal stressor (Lindley & Galupo, 2020), it may be beneficial to develop interventions that not only address the experience of dysphoria itself but also target the broader social conditions that may contribute to or exacerbate it. These could include efforts to improve access to gender-affirming healthcare services and to reduce stigma and marginalization against transgender individuals in both clinical and societal settings. Moreover, considering the buffering role of resilience, it may be valuable to integrate resilience-building strategies, such as fostering self-acceptance and emotion regulation, into mental health programs and community-based initiatives. Although not directly examined in the current study, promoting additional dimensions of resilience, including social support and community connectedness, may also bring about favorable outcomes, as various forms of resilience are interrelated and can reinforce one another (Puckett et al., 2024b).
Despite the aforementioned findings, several limitations of the present study should be considered when interpreting and applying the results. First, the cross-sectional nature of this study does not permit conclusions about causality. Longitudinal research is therefore needed to examine the relationships between variables over time. Second, the relatively small and demographically limited sample, characterized by a high proportion of binary-identified, low-income, and undergraduate participants, may limit the generalizability of the findings. The bias in sampling methods may help explain why most effect sizes observed in this study were small to moderate. Third, the use of an online survey may have inadvertently excluded transgender individuals without internet access. Although rigorous data quality control procedures were implemented (e.g., allowing only one response per email address, verifying consistency between sex assigned at birth and gender identity), duplicate or erroneous entries cannot be entirely ruled out. Fourth, while definitions for less commonly understood terms (e.g., “gender identity,” “affirmed gender”) were provided, participants might still have interpreted these terms differently, potentially introducing bias or error into their responses. Lastly, although this study was grounded in the Minority Stress Model (Meyer, 2003), it did not account for cultural factors specific to the Vietnamese context (e.g., collectivism or awareness of gender equality). The absence of these culturally relevant variables may have limited the explanatory power of the findings and the potential for cross-cultural comparison.
CONCLUSIONS
This study contributes to the growing body of literature on transgender mental health by providing empirical evidence from the Vietnamese context, where transgender rights are still in the process of gaining broader recognition within legal and social frameworks. Both gender dysphoria and psychological distress emerged as prevalent concerns among transgender individuals in Vietnam, with their levels varying across sociodemographic groups. The positive association between gender dysphoria and psychological distress supports the notion that gender dysphoria may function as a proximal stressor specific to transgender populations. Notably, consistent with the Minority Stress Model, resilience was found to buffer the adverse psychological effects of gender dysphoria. These findings underscore the potential value of mental health approaches that not only address the experience of dysphoria itself but also foster resilience to improve the overall well-being of transgender individuals.