BACKGROUND
The World Health Organization persistently emphasizes the importance of promoting a healthy lifestyle (WHO, 2020). Healthy eating and physical activity become particularly important during pregnancy, because this period affects both women and their future children (Maciąg et al., 2013; Phelan, 2010). Moreover, pregnancy may create a window of opportunity to initiate behavioral changes (Phelan, 2010). However, pregnancy is also characterized by challenges stemming from sudden changes in many aspects of women’s lives which simultaneously overwhelm physical, hormonal, and mental functioning (Kazma et al., 2020; Qiu et al., 2012; Soma-Pillay et al., 2016).
In challenging situations, self-control is engaged (Hagger et al., 2010; Muraven et al., 2006). Resource depletion theory states that the more individuals use certain internal resources, the faster their self-control becomes depleted (Baumeister et al., 1998; Clinton et al., 2020; Hagger et al., 2013). A decrease in the ability to control one’s own internal states and behaviors may cause difficulties in maintaining health behaviors (Bai et al., 2021; Baumeister et al., 1994; Inzlicht et al., 2020; Soma-Pillay et al., 2016).
As rapid and challenging changes during pregnancy deplete self-control (Hagger et al., 2010; Muraven & Baumeister, 2000; Van Scheppingen et al., 2018), we hypothesized that the third trimester of pregnancy is the hardest in terms of maintaining healthy behaviors. At the end of pregnancy, women may often use the least efficient, but the easiest forms of self-regulation such as compensatory health beliefs (Knäuper et al., 2004). These are beliefs that the negative effects of unhealthy behavior can be compensated for or neutralized by engaging in healthy behavior (Knäuper et al., 2004, p. 607).
In this research, we hypothesized that pregnancy is conducive to the depletion of self-control resources, because it is a time when self-regulation is put to the test by difficulties associated with dynamic changes in the body and mind. More succinctly, we hypothesized that self-control decreases as pregnancy progresses. As a consequence, we expected that pregnant women would opt for simpler forms of self-regulation, such as compensatory beliefs. It is much easier to form a belief than to compensate for unhealthy behavior with a healthy option (Festinger, 1957; Rabiau et al., 2006). The more self-control is depleted in a tempting situation, the greater is the likelihood that compensatory health beliefs will emerge, and the less likely it is that a person will engage in compensatory behaviors or resist temptations (Rabiau et al., 2006).
PSYCHOLOGICAL AND PHYSIOLOGICAL ASPECTS OF PREGNANCY
Pregnancy is a demanding period full of joy but also doubts, anxiety and fear (Barbu et al., 2020; Essen et al., 2000; Maciąg et al., 2013). It is characterized by physical pain, difficulties with sleep, and restrictions in sexual life (Bao et al., 2020; Majchrzycki et al., 2010; Polo-Kantola et al., 2017; Sharma & Franco, 2004). The nature of the challenges changes over the three trimesters.
The first trimester (1-3 months, 1-13 weeks of pregnancy) is dominated by physiological changes, both hormonal and physical (Bjelica et al., 2018; Wojaczek, 2012). Ailments such as nausea, vomiting, headaches, breast pain, and drowsiness are often present (Sacomori & Cardoso, 2010). This stage of pregnancy is also characterized by anxiety and fear related to childbirth and the risk of losing the pregnancy (Sacomori & Cardoso, 2010). During this time, the woman is focused on herself and the changes in her body (Boscaglia et al., 2003; Inanir et al., 2015).
In the second trimester of pregnancy (4-6 months, 14-27 weeks of pregnancy) the unpleasant experiences of the first trimester, such as nausea, pass, allowing full concentration on the baby (Chan et al., 2011). However, it is only relatively easy, as changes are still taking place in the woman’s body as it is exposed to cumulative effort (Newham & Martin, 2013). Weight gain, swelling, changes in the myofascial system, and back pain confirm that the changes at this stage of pregnancy are constantly taking place (Fraś et al., 2012; Opala-Berdzik et al., 2009; Saptyani et al., 2020; Urtnowska et al., 2015).
The third trimester (7-9 months, 28-39/40 weeks of pregnancy) is the period of pregnancy during which the strongest emotional bond between the mother and child is built Wojaczek, 2012). However, mood instability, emotional sensitivity, and mental exhaustion become more common (Barbu et al., 2020). Concern and anxiety reappear due to approaching childbirth and anticipation of pain, fears of complications, as well as fears about the health and safety of the women themselves and their children (Bielawska-Batorowicz, 2006; Lichtenberg-Kokoszka, 2008; Nekoee & Zarei, 2015). Anxiety increases in the third trimester compared to the first and the second (Salafas et al., 2020). Negative feelings are also associated with the already visible physical changes, such as the increase in the woman’s body weight. A large belly causes more fatigue, and problems with breathing, moving, and changing position (Franklin & Conner-Kerr, 1998; Majchrzycki et al., 2010). Back pain, swelling, constipation, feeling of shortness of breath, and heaviness may also occur (Davis, 1996; Majchrzycki et al., 2010; Wojaczek, 2012). Moreover, sleep disorders such as insomnia are also more likely in the third trimester of pregnancy (Neau et al., 2009; Salari et al., 2021). Due to these many changes in the woman’s body, and psychological functioning, pregnancy poses a challenge to self-regulatory processes.
SELF-CONTROL DEPLETION AND SELF-CONTROL AS A TRAIT
Self-regulation refers to the broader process of guiding behavior towards a desired goal and includes goal setting, monitoring progress in achieving goals, and acting in accordance with goals (Carver & Scheier, 2003; Gillebaart, 2018; Inzlicht et al., 2020). Self-control is an ability to resolve conflicts between goals that provide an immediate reward (desires that bring immediate fulfillment) and long-term goals, which require delayed gratification (Ainslie, 1974; Duckworth et al., 2016; Fujita, 2011). Self-control enables, facilitates, and maintains the pursuit of important goals (Baumeister & Heatherton, 1996). For example, when choosing between a delicious dessert and a healthy salad, self-control is used to resolve the conflict between the short-term goal of eating delicious food and the long-term goal of being healthy and fit.
According to the resource depletion model, self-control is defined as the ability to overcome undesirable behaviors (Tangney et al., 2004). Self-control resources intensify in the face of factors that reduce the chances of achieving a goal (Vohs & Baumeister, 2004). However, these resources are limited and diminish with use. Self-control weakens over time, so that less and less effort is made with each successive task requiring control (Baumeister et al., 1998). Weakened self-control reduces the ability to refrain from temptations and achieve goals, such as maintaining a healthy diet (Muraven & Baumeister, 2000). Accordingly, the basis of behavioral regulation in this approach is the inhibition of impulses.
Individuals differ in the extent to which they manage to deal with obstacles and hurdles when pursuing their goals (Sorys et al., 2023). Individuals with high levels of trait self-control are more successful in resisting temptations, inhibiting or altering impulses, and overriding undesired behavioral tendencies (Baumeister, 2002; Milyavskaya et al., 2015; Tangney et al., 2004; Vosgerau et al., 2020). Trait self-control, as a personality trait, affects the frequency and intensity of certain forms of behavior, such as resisting temptations, suppressing undesirable impulses, and postponing the immediate satisfaction of needs for more distant or socially approved gratification (Baumeister & Heatherton, 1996; Ent et al., 2015; Hofmann et al., 2012, 2013; Tangney et al., 2004; Trope & Fishbach, 2000). Buczny and Międzyobrodzka (2014) assume that the effects of depletion of self-control resources are lower among those with higher compared to those with lower self-control as a trait.
COMPENSATORY HEALTH BELIEFS AS A SELF-REGULATION STRATEGY
Individuals strive to achieve a balance between the fulfillment of desires and the pursuit of their important goals. Sometimes, however, a motivational conflict arises between short-term desires and long-term health goals (Rabiau et al., 2006). According to the compensatory health beliefs model, such conflicts can be attenuated in three ways: by resisting a temptation (Baumeister & Heatherton, 1996; Giner-Sorolla, 2001), changing one’s perception of an expected outcome (Baumeister et al., 1994) or formulating compensatory health beliefs (Rabiau et al., 2006). Formulating compensatory health beliefs means that a person comes to believe that the maladaptive effects of unhealthy behavior can be compensated for or neutralized by a recovery plan, which involves later engagement in healthy behavior (Knäuper et al., 2004).
Compensatory health beliefs are more likely to be relied upon when the desired behavior is hard to resist (Norman et al., 1999). They can help resolve the dilemma between immediate pleasure and guilt stemming from not pursuing an important goal (Rabiau et al., 2006). They give permission to eat unhealthy food or to be inactive without feeling guilt and discomfort (Giner-Sorolla, 2001; Knäuper et al., 2004; Sorys & Byrka, 2021). Compensatory health beliefs can be considered effortless self-regulatory strategies that people fall back on when they are unable to resist a temptation (Knäuper et al., 2004). In this way, people soothe their consciences and justify succumbing to desires (Obara-Gołębiowska & Michałek, 2015). Nonetheless, reliance on compensatory beliefs inhibits success in maintaining healthy behaviors. Previous research has shown that falling back on compensatory beliefs translates into higher calorie diets (Rabiau et al., 2009), a diminished ability to quit smoking (Radtke & Scholz, 2012), and a reduced likelihood of being vaccinated (Ernsting et al., 2013).
RESEARCH GOALS
Pregnancy is characterized by rapid changes, and physical and mental challenges (Barbu et al., 2020; Essen et al., 2000; Maciąg et al., 2013). Due to the depletion of self-control resources, in such a challenging period, we hypothesized that levels of self-control would decrease during pregnancy, from the first to the third trimester (hypothesis 1). Past research has shown that the decrease in self-control resources results in an increase in the level of compensatory beliefs, i.e., self-regulation strategies that disturb healthy functioning (Rabiau et al., 2006). Accordingly, the frequency of compensatory health beliefs in different life domains such as nutrition or substance abuse should increase over the course of pregnancy, being the most frequent in the third trimester (hypothesis 2). We also assumed a positive relationship between self-control and compensatory health beliefs (hypothesis 3). We expected that when their levels of self-control decrease, pregnant women give themselves greater permission to eat, and in situations where they feel remorse for eating excess food, they will use compensatory health beliefs (Glock et al., 2013; Knäuper et al., 2004; Matley & Davies, 2018; Zhao et al., 2021). Therefore, we expected that compensatory health beliefs in the third trimester of pregnancy would mediate the relation between trait self-control measured in the first trimester and unhealthy snacking habits in the third trimester (hypothesis 4).
PARTICIPANTS AND PROCEDURE
PARTICIPANTS
Initially, 169 women volunteered to take part in the study and fulfilled inclusion criteria, that is being adult (18 years old) and in the first trimester of pregnancy. Out of 169 participants, three dropped out after the completion of the first measurement (t1). Finally, data from 166 women who completed all free measurements (t1, t2, t3) were considered for the analysis in the study (drop-out 1.8%). Since the drop-out was marginal and the quality of data was very good, we did not employ any data imputation methods. Listwise deletion was used for all analyses, except for the linear-mixed effects.
The participants were patients from hospitals, private gynecological practices, and health and dental clinics; participants in antenatal classes; students of the Higher School of Safety; and members of beauty salons in Silesia, Poland in the period from April 2019 to July 2020.
The oldest participant was 44, the youngest 19 years old (M = 28.74, SD = 5.53). The vast majority of the women had secondary (41.0%) or higher (44.6%) education. It is also worth noting that most of the participants were pregnant for the first (77.6%), second (25.3%), third (14.5%), fourth (4.8%), fifth (2.4%), and sixth (1.2%) time. For the remaining 4.2% there are no data.
A formal power analysis was not conducted prior to the study. The first measurement was part of a larger cross-sectional study. Women in the first trimester were invited to the longitudinal study described in this paper. Since this project did not have any institutional funding, the number of participants was limited by the organizational capacities of the authors.
STUDY DESIGN AND PROCEDURE
In this longitudinal study, participants completed the questionnaires in the first, second and third trimesters of pregnancy. The following variables were examined: compensatory health beliefs, self-control, the week and trimester of pregnancy, and unhealthy snacking habits. The first measurement was made personally by the researcher, while the other measurements were carried out electronically. The average number of days between measurements t1 and t2 equaled M = 57.73, SD = 19.64 (ranging from 18 to 106 days) and for measurements t2 and t3 it was M = 77.22, SD = 26.05 (ranging from 22 to 164 days).
The procedure was not approved by the ethics review board prior to the study, but the study followed good practices in the discipline.
First trimester (t1). Before the first measurement, the participants read instructions and gave written consent to participate in the study. They were also informed about the possibility of discontinuing participation at any time. Each participant then completed a questionnaire in which they provided their demographic information, weight, information on the week and trimester of pregnancy, and e-mail so they could be contacted if they expressed their willingness to participate in the next stages of the study. Then, they provided responses to questions about compensatory health beliefs, self-control, and self-control regarding eating. Confidentiality was maintained, and data were treated with utmost care. The first measurement was part of a larger project. Not all analyses will be presented in this article.
Second trimester (t2). In the second measurement (t2), participants responded to questions about the trimester and week of pregnancy, self-control and compensatory health beliefs.
Third trimester (t3). In the third measurement (t3), participants answered questions about the trimester and week of pregnancy, self-control, and compensatory health beliefs. In addition, unhealthy snacking habits were measured.
MEASURES
Compensatory health beliefs were measured with the Polish version of the compensatory health beliefs scale (Knäuper et al., 2004). The scale was translated into Polish with the consent of the authors by Obara- Gołębiowska and Michałek (2015). It is a general measure of health beliefs consisting of 17 items in four dimensions: 1) Compensation for the effects of substance use, e.g., “Smoking can be compensated for by exercising”. 2) Compensating for unhealthy eating and sleeping habits e.g., “Eating whatever one wants in the evening is OK if one did not eat during the entire day”. In this study, only items related to compensating for unhealthy eating habits from the second dimension were analyzed. Sleep was not included in the analyses to keep the focus exclusively on unhealthy eating. 3) Compensation for the effects of stress, e.g., “A stressful day can be compensated for by relaxing in front of the TV”. 4) The fourth factor is related to the regulation of body weight, e.g., “Eating dessert can be made up for by skipping the main dish”. Answers were scored on a five-point Likert scale, from 1 (strongly disagree) to 5 (strongly agree). The reliability of the scale was assessed on the basis of Cronbach’s α internal consistency coefficient and was α = .79 in the first measurement (t1), α = .79 in the second measurement (t2), and α = .70 in the third measurement (t3).
Trait self-control was measured using the Polish version (Buczny & Międzyobrodzka, 2015) of the Trait Self-Control Scale (Tangney et al., 2004), which consists of 13 items. Exemplary items include “I am effective at resisting temptations” and “Pleasures and distractions make it difficult for me to complete tasks”. Items were responded to on a five-point Likert scale, from 1 (strongly disagree) to 5 (strongly agree). The reliability of the questionnaire was assessed on the basis of Cronbach’s α internal consistency coefficient and was α = .73 in the first measurement (t1), α = .79 in the second measurement (t2), and α = .84 in the third measurement (t3).
Unhealthy snacking habits was measured at t3 only with the Polish version (Łuszczyńska et al., 2013) of the Self-Report Habit Index (Verplanken & Orbell, 2003), which consists of 12 items. In this study, six items, as selected by Łuszczyńska et al. (2013), were used to measure succumbing to food temptations among pregnant women. Examples are as follows “Eating unhealthy snacks is something I do automatically” and “Eating unhealthy snacks is something that would require effort not to do”. Items were responded to on a five-point Likert scale from 1 (never) to 5 (very often). The internal consistency of the scale was α = .94. The items in the tool contain two basic elements of habits: frequency and automatism. They can be supplemented with an example of any behavior, depending on the purpose of the study (Verplanken & Orbell, 2003).
RESULTS
LEVEL OF SELF-CONTROL AND THE TRIMESTER OF PREGNANCY
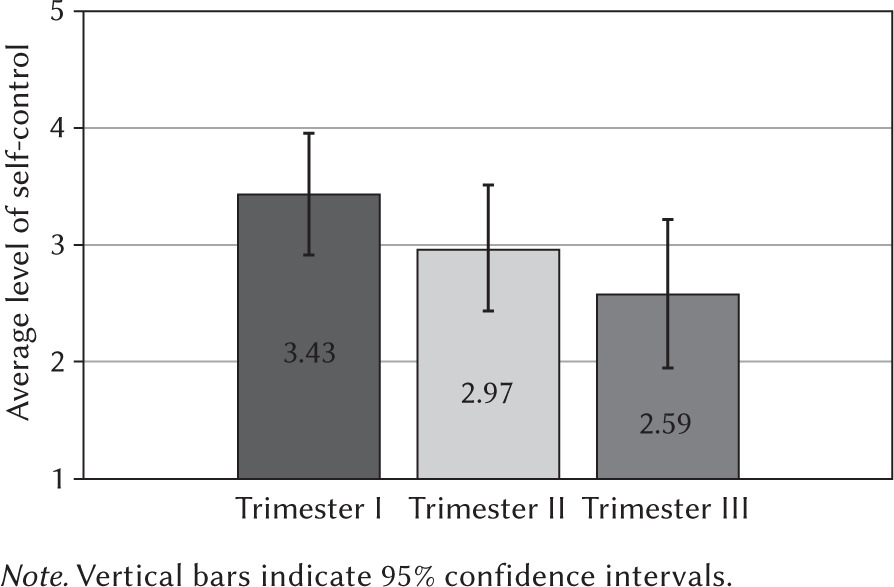
A mixed-effects analysis of variance with self-control measured at three points as a within-subject factor showed the main effect of measurement, F(1.4, 237) = 275.97, p < .001, η2 = .63) (hypothesis 1). Due to the violation of the assumption of the sphericity of variance, the Greenhouse-Geisser correction was imposed on the results of the analysis. Post-hoc tests showed that women in their first trimester (t1) (M = 3.43, SD = 0.53, 95% CI [3.35; 3.51]) reported a higher level of self-control compared to those in their second trimester (t2) (M = 2.97, SD = 0.54, 95% CI [2.89; 3.05], t(165) = 14.06, p < .001, d = 1.09, 95% CI [0.90; 1.28]) and third trimester (t3) (M = 2.59, SD = 0.63, 95% CI [2.50; 2.69], t(165) = 18.52, p < .001, d = 1.44, 95% CI [1.22; 1.65]). Women in their second trimester (t2) reported significantly higher self-control compared to the third trimester (t3) (M = 2.59, SD = 0.63; 95% CI [2.50; 2.69], t(165) = 14.16, p < .001, d = 1.10, 95% CI [0.91; 1.29]. The results are presented graphically in Figure 1.
LEVEL OF COMPENSATORY HEALTH BELIEFS AND TRIMESTER OF PREGNANCY
In the second step of the analysis, we tested whether levels of compensatory health beliefs were dependent on the time of measurement, that is, the trimester of pregnancy. We performed a mixed-effects analysis of variance. Due to the violation of the assumption of the sphericity of variance, the Greenhouse-Geisser correction was again imposed on the results of the analysis.
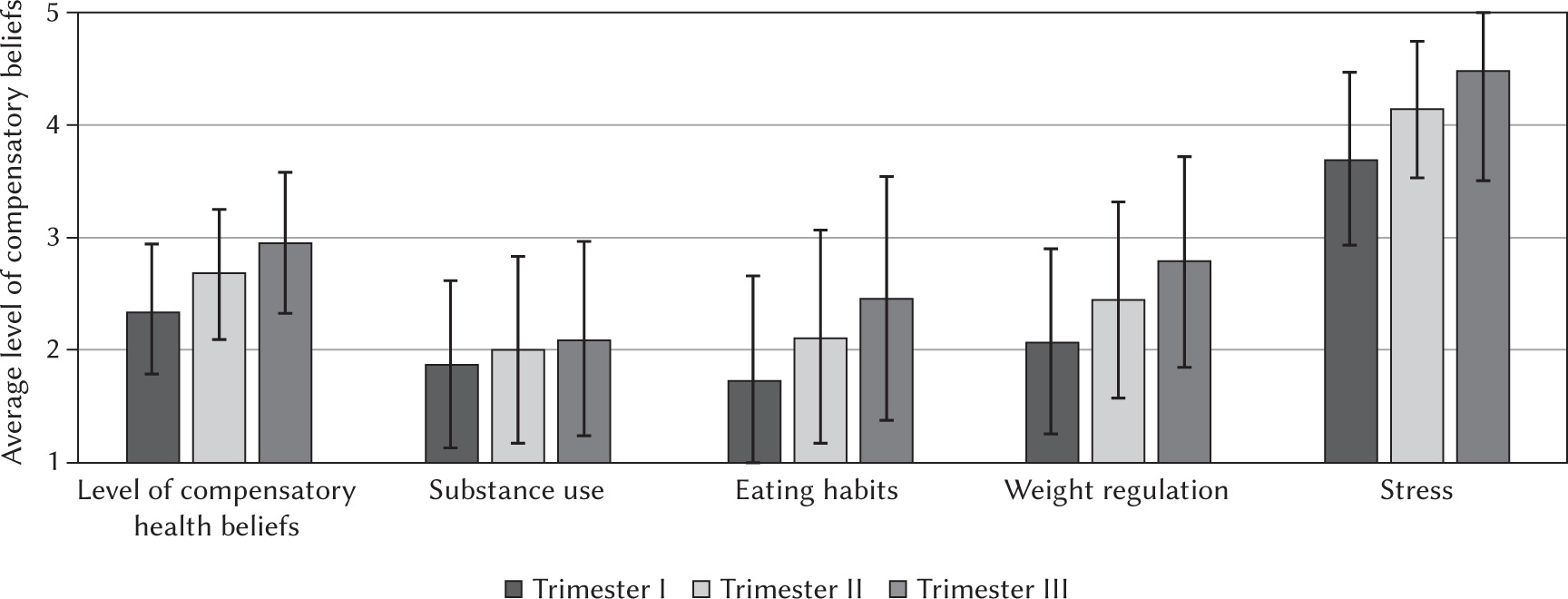
We observed the main effect of the time of measurement on the level of compensatory health beliefs, F(1.5, 249.10) = 188.05, p < .001, η2 = .53. Women in their first trimester (t1) reported compensatory health beliefs less frequently (M = 2.34, SD = 0.57, 95% CI [2.25; 2.43]) compared to those in the second trimester (t2) (M = 2.67, SD = 0.58, 95% CI [2.58; 2.76], t(165) = –11.73, p < .001, d = –0.91, 95% CI [–1.09; –0.73]) and third trimester (t3) (M = 2.95, SD = 0.63, 95% CI [2.85; 3.04], t(165) = –15.05, p < .001, d = –1.2, 95% CI [–1.40; –1.00]). Women in the second trimester (t2) reported lower levels of compensatory health beliefs compared to those in their third trimester (t3) (M = 2.95, SD = 0.63, 95% CI [2.85; 3.04], t(165) = –11.10, p < .001, d = –0.86, 95% CI [–1.04; –0.68]).
Consistent results were observed for all dimensions of compensatory health beliefs. We observed main effects of the time of measurement on substance use (F(1.56, 257.77) = 36.19, p < .001, η2 = .18), eating habits (F(1.67, 275.51) = 88.21, p < .001, η2 = .35), weight regulation (F(1.4, 230.17) = 105.77, p < .001, η2 = .39), and stress (F(1.39, 228.73) = 60.98, p < .001, η2 = .27).
The analysis showed that with the increase of trimester came increases in the levels of each of the examined compensatory subdimensions of health beliefs. Notably, the effect size observed in the third trimester (t3) was the strongest. Detailed results of the analyses are presented in Figure 2.
RELATIONSHIP BETWEEN COMPENSATORY HEALTH BELIEFS AND SELF-CONTROL AS A FUNCTION OF THE TRIMESTER OF PREGNANCY
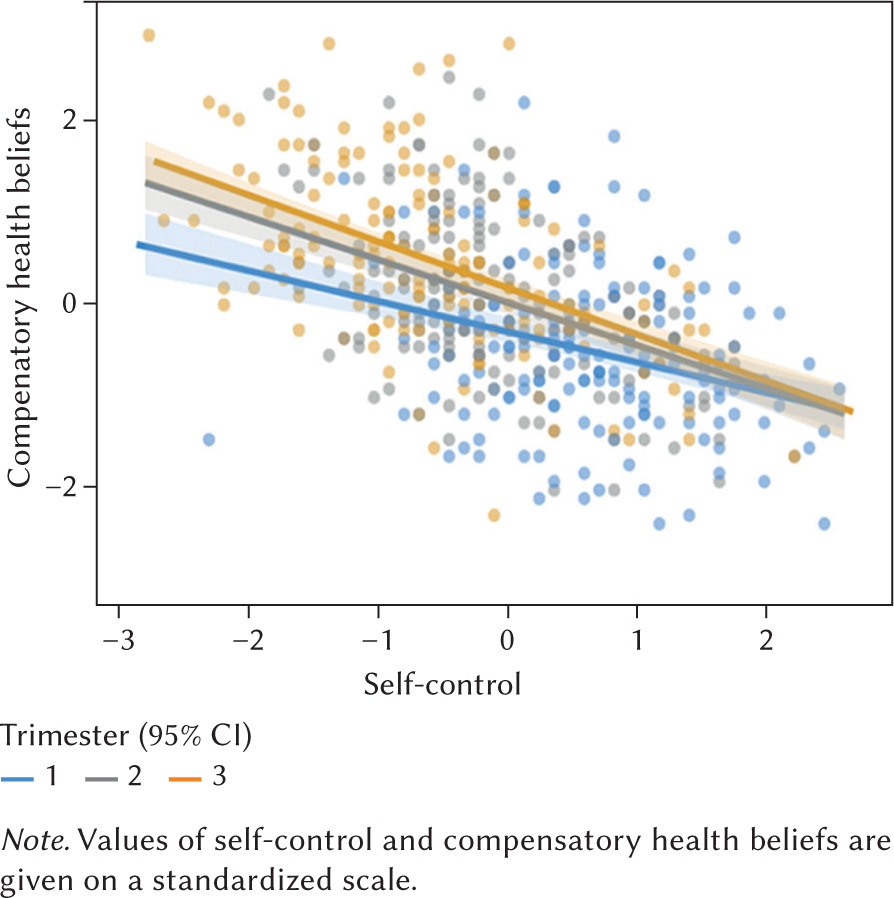
We performed a linear mixed-effects analysis to test the effects of self-control on compensatory health beliefs at different stages of pregnancy. We introduced random intercepts to the model. The results revealed a main effect of self-control on compensatory behaviors, F(1, 464) = 145.21, p < .001, a main effect of the time of measurement, F(2, 364) = 25.88, p < .001, and more interestingly, an interaction between self-control and the stage of pregnancy, F(2, 337) = 6.71, p < .01.
The relation between self-control and compensatory health beliefs was the strongest in the third trimester (t3) (β = –.51, SE = .04, 95% CI [–.59; –.43], t = –9.46, p < .001) and the weakest in the first (t1) (β = –.33, SE = .05, 95% CI [–.43; –.24], t = –12.32, p < .001). The strength of the effect in the second trimester (t2) was between strengths of the first (t1) and the third (t3) (β = –.47, SE = .05, 95% CI [–.57; –.37], t = –7.12, p < .001). This suggests that self-control may play the role of a buffer that is particularly needed when resources are the most depleted, that is, in the third trimester (t3). See Figure 3.
THE MEDIATING ROLE OF COMPENSATORY HEALTH BELIEFS IN THE RELATIONSHIP BETWEEN SELF-CONTROL AND UNHEALTHY SNACKING HABITS
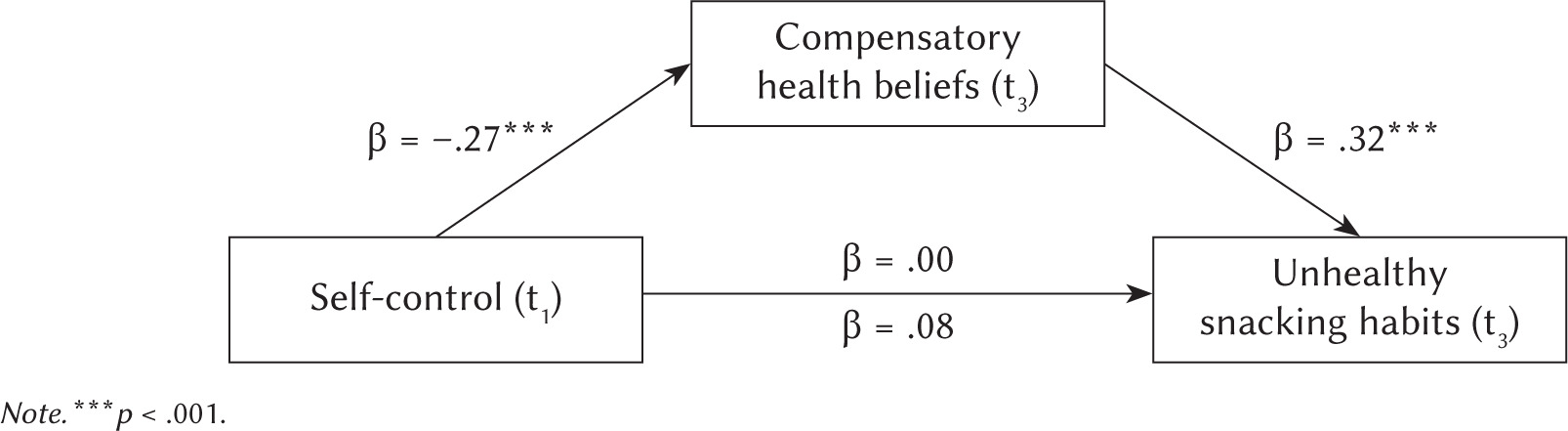
To address hypothesis 4, we performed a mediation analysis (PROCESS Model 4; Hayes & Scharkow, 2013) in which compensatory health beliefs in the third trimester (t3) mediated (M) the relationship between the level of self-control (X) in the first trimester (t1) and the level of unhealthy snacking habits (Y) in the third trimester (t3).
The results showed significant paths from self-control to compensatory health beliefs (β = –.33, SE = .09, 95% CI [–.50; –.15], t = –3.64, p < .001) and from compensatory health beliefs to unhealthy snacking habits (β = .40, SE = .10, 95% CI [.21; .59], t = 4.15, p < .001). More importantly, the indirect effect of compensatory health beliefs was significant (β = –.09; SE = .03, 95% CI [–.16; –.03]). Detailed results are presented in Figure 4.
Figure 4
Standardized regression analysis coefficients revealing the effectiveness of the level of compensatory health beliefs (third trimester – t3) as a mediator of the relationship between the level of self-control (first tr mester – t1) and the level of unhealthy snacking habit (third trimester – t3)
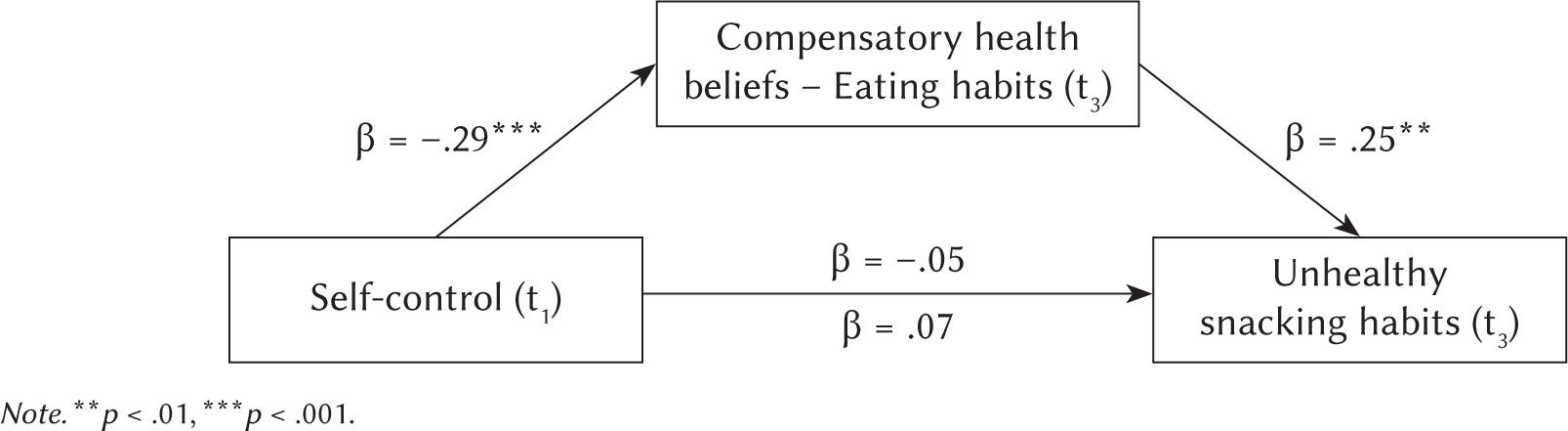
THE MEDIATING ROLE OF EATING HABITS AS ONE OF THE COMPENSATORY EATING BELIEFS IN THE RELATIONSHIP BETWEEN SELF-CONTROL AND UNHEALTHY SNACKING HABITS
We additionally performed a mediation analysis (PROCESS Model 4; Hayes & Scharkow, 2013) in which eating habits in the third trimester (t3) mediated (M) the relationship between the level of self-control (X) in the first trimester (t1) and the level of unhealthy snacking habits (Y) in the third trimester (t3).
The results showed significant paths from self-control to eating habits (β = –.59, SE = .15, 95% CI [–.89; –.29], t = –3.87, p < .001) and from compensatory eating beliefs to unhealthy snacking habits (β = .19, SE = .06, 95% CI [.07; .30], t = 3.19, p = .002). More importantly, the indirect effect of compensatory eating beliefs was significant (β = –.07, SE = .03, 95% CI [–.14; –.02]). Detailed results are presented in Figure 5.
DISCUSSION
This research focused on the dynamics of self-regulatory processes in women over the course of their pregnancies. The study showed that pregnant women are at risk of self-regulation failures resulting from the exhaustion of self-control. Self-control as an individual trait decreased as pregnancies progressed (hypothesis 1). In line with the resource depletion theory, as the time in the demanding state of pregnancy passed, trait self-control decreased (Baumeister et al., 1998). These findings extend past research on resource depletion, showing that this process can occur over periods as long as a couple of months.
Previously, research by Francis et al. (2021) showed that individuals are more likely to be prosocial and empathetic in the morning than in the evening as the demands of the day deplete self-control. It appears that pregnant women control their behaviors more in the early stage of pregnancy, as they are aware that their actions affect both their health and the proper development of their future children (Phelan, 2010). Self-regulatory exhaustion by the end of pregnancy may result from situational factors (Lefevor et al., 2017) and individual changes (Habashi et al., 2016).
As predicted, levels of compensatory health beliefs increased as pregnancies progressed (hypothesis 2). Both the overall level of compensatory beliefs and the level of compensatory beliefs in each of the four dimensions increased. The strongest effect was observed in the dimension of body weight and unhealthy eating habits, and the weakest change was observed in substance use. These results are in line with the existing research. According to Fairburn et al. (1992) and Hill et al. (2016), concerns regarding food consumption increase over the course of pregnancy. One strategy used to alleviate this state of discomfort is the activation of compensatory health beliefs (Rabiau et al., 2006). An individual may believe that the negative effects of weakness and unhealthy snacking can be compensated for by subsequent healthy behavior.
Rabiau et al. (2006) argued that individuals opt for compensatory beliefs when they face challenges to their self-control. Our results confirm the relationship between compensatory health beliefs and self-control (hypothesis 3). With the decrease of trait self-control in the first, second, and third trimesters the level of compensatory health beliefs increased as well. Interestingly, the relation between self-control and compensatory health beliefs was the strongest in the third trimester reveling large effect sizes (Cohen, 1962). The less self-control the participants reported, the more frequently they formulated compensatory health beliefs. In other words, greater self-control served as a buffer to the use of more efficient self-regulatory strategies rather than compensatory beliefs. Future research should examine what types of self-regulatory strategies pregnant women with high trait self-control adopt when exhausted.
Compensatory health beliefs are classified as maladaptive health beliefs because they are used to justify unhealthy behavior. Moreover, the formulation of a compensatory belief may block the implementation of a compensatory behavior, and it may reduce the likelihood that a person will engage in a healthy behavior (Knäuper et al., 2004). They also prevent effective compliance with changes in maintaining health, e.g. in refraining from caloric intake or quitting smoking (Radtke & Scholz, 2012). Rabiau et al. (2006) suggested that having many compensatory beliefs can have a negative impact on health (Knäuper et al., 2004). This study showed that lower trait self-control among pregnant women in the first stage of pregnancy translates into compensatory health beliefs at the end of pregnancy. This, in turn, translates into higher chances of snacking and unhealthy food consumption (hypothesis 4).
We observed consistent results both when including general compensatory health beliefs and compensatory eating beliefs as mediators. In fact, the effect of general compensatory health beliefs on unhealthy snacking was stronger than the effect of compensatory eating beliefs. This is probably due to the better quality of the comprehensive measure compared to the shorter subscale. Individual levels of self-control at the beginning of pregnancy carried over into the final stage. Future research should verify the behavior of pregnant women, rather than simply relying on declarations of behavior, as in this study. When interpreting these results, however, one should bear in mind that unhealthy snacking habits were measured only at the last stage of pregnancy. We could not control for the level of snacking at the beginning of pregnancy, so might not be fully certain about the causal path observed. Nonetheless, the proposed causation order in the mediation model is theoretically grounded.
Compensatory health beliefs do not actually compensate for self-regulatory failures (Knäuper et al., 2004). It is worth intervening at the stage of activation of compensatory beliefs and motivating pregnant women to implement planned compensatory behaviors after self-regulatory failures. Specific action plans can be developed and worked through with pregnant women (Gollwitzer, 1999). Moreover, interventions focused on enhancing self-efficacy could also be effective in converting compensatory health beliefs into compensatory behaviors (Luszczynska et al., 2007; Nguyen et al., 2006). Research conducted by Obara-Gołębiowska (2016) among patients in an obesity treatment ward confirmed that higher self-efficacy was related to less frequent compensatory health beliefs. Future research should also examine compensatory health beliefs specific for pregnancy, such as self-testing, monitoring of the child’s development, and regular check-ups, as these compensatory health beliefs might hinder behaviors specific for pregnancy only.
Self-regulatory failures and decreased self-control are also likely after the birth of a child, as this period is demanding, especially after a difficult birth for example, through cesarean section (Prokopowicz et al., 2021). Maintaining a healthy lifestyle is challenging in the postpartum stage because women must simultaneously cope with the new role of motherhood in the best possible way and aim to return to their pre-pregnancy lifestyle.
CONCLUSIONS
Trait self-control is of importance for the formation of compensatory beliefs, especially towards the end of pregnancy, as its level is then at its lowest. The more the level of trait self-control decreases in pregnant women, the more often they display maladaptive compensatory health beliefs. The level of self-control a pregnant women has at the beginning of pregnancy also determines how often she formulates compensatory health beliefs. In turn, a high level of compensatory health beliefs means that pregnant women are more likely to take up unhealthy snacking habits, which confirms that compensatory beliefs are not effective forms of self-regulation.
From the theoretical point of view, our results confirm assumptions of the resource theory showing that self-control depletes when individuals confront challenges. Interestingly, not only situational self-control, but also a relatively stable trait changed in a few-month period of time. From the applied point of view, our results encourage working with pregnant women, educating them, and intervening in order to strengthen their self-control and self-regulation strategies that increase the likelihood of achieving health-oriented goals.