BACKGROUND
The Global Burden of Disease Study 2019 report shows that self-harm and depressive disorders are the third and fourth ranking causes of disability-adjusted life-years (DALYs) for the 10-24-year-old group (GBD 2019 Diseases and Injuries Collaborators, 2020). The result is supported by other studies describing the phenomenon of depressive disorders among university students, ranging from 23.8% to 35%, both in developed and developing countries (Beiter et al., 2015; Lei et al., 2016; Othieno et al., 2014; Sheldon et al., 2021). In Indonesia, the prevalence of depression among the general population is 6.1% (Ministry of Health of the Republic of Indonesia, 2019), but the prevalence among university students is predicted to be higher, ranging from 18.8% (Marthoenis et al., 2018) to 25% (Astutik et al., 2020). Although substantial heterogeneity in prevalence estimates of depression is also noted because of different assessment tools used and varying quality of different studies (Chen et al., 2013; Ibrahim et al., 2013), depression among university students still be a burden and high risk of suicidal behavior (Akram et al., 2020; Gselamu & Ha, 2020). Unidentified depression, especially when severe, can increase the probability of having suicidal behavior. Therefore, better understanding of the mechanism of depression could help develop more effective intervention to prevent suicide among university students.
Previous studies have shown that the risk for developing depression tends to increase when individuals had adverse childhood experiences (ACEs) in their earlier life. Having experienced 3 or more types of adversity during childhood increases the likelihood of having depression (OR = 1.81, p = .002) and having made suicide attempts (OR = 3.31, p < .001) compared to those without adversity experience (He et al., 2021). Another study of 4675 undergraduate university students from Cambodia, Indonesia, Malaysia, Myanmar, Thailand and Vietnam showed that the overall prevalence of ever suicidal ideation and ever suicide attempt among students in this study was 11.7% and 2.4%, respectively (Peltzer et al., 2017). In Indonesia alone, out of 321 participants, 6.9% had had suicidal ideation while 3% had made a suicide attempt. History of adverse childhood experiences is taken into consideration in that study. Having childhood maltreatment experience also significantly predicts both new onset and recurrent depressive disorders (Hovens et al., 2015), earlier onset and higher severity of depression, and higher resistance to depression treatment (Nelson et al., 2017). The indirect association is mediated positively by current stressful events (Kelifa et al., 2020), emotion dysregulation and negative internalized belief (Coates & Messman-Moore, 2014), and dysfunctional attitude (negative attitude towards self, outside world, and the future) (Ju et al., 2020), and negatively by resilience (Vieira et al., 2020) and mindfulness (McKeen et al., 2021).
ACEs and the following consequences of it indicate the difficulty to forgive among those experiencing them. Carrying wounds after having experienced childhood adversities impacted on reduced hippocampal and amygdala volume, and increases stress sensitivity and risk for having depression (Weissman et al., 2020). Forgiveness is defined as a positive psychological attribute, which involves reframing events that are considered to have been violating, whether the perpetrator is oneself, others, or situations, as well as the sequelae of the violation, to be changed from negative to neutral or positive (Thompson et al., 2005). Regarding forgiveness among individuals with ACEs, a study by Mojallal et al. (2021) found that neglect, sexual abuse, and punishment were associated with proneness to shame and guilt, which indicated the need of forgiveness, specifically self-forgiveness. Likewise, individuals with ACEs who practice forgiveness are also found to have better physical health (Banyard et al., 2017).
Studies in the context of ACEs regarding forgiveness that covers all three dimensions and its relationship to depression – including how it mediates and moderates – are still limited. One study conducted by Arslan (2017) found that forgiveness as an accumulation of three dimensions in those with a history of ACEs mediated the relationship of psychological maltreatment with a mental health problem, but in this case internet addiction, which in other literature has consistently explained the positive relationship between internet addiction and depression (e.g. Liang et al., 2016). Meanwhile, another previous study by Ramsey (2019), which used a forgiveness scale containing three dimensions (Thompson et al., 2005), resulted in unique moderations (based on the dimensions) in the relationship between ACEs and the emergence of psychological problems including depression. Other forgiveness studies in the context of ACEs and depression do not use forgiveness as an accumulation of three dimensions, such as that conducted by Wu et al. (2019), which found that self-compassion as well as trait forgiveness (in this case specifically towards others) moderated the effect of ACEs on depression.
Despite the limited number of previous studies above, other studies describe forgiveness as a mediator or moderator in relation to depressive symptoms outside the specific context of ACEs. A systematic review of 18 studies by Cleare et al. (2019) found that there were significant negative correlations between self-compassion or forgiveness (specifically self-forgiveness) and self-harm or suicidal ideation with some indication that self-compassion or self-forgiveness might buffer the relationship between negative life events and self-harm. Hirsch et al. (2012) also found that self-forgiveness served as a significant moderator between anger expression and suicidal behavior, particularly in weakening the association between the two variables.
As researchers have tried to describe above, in addition to potentially mediating the relationship between ACEs and depression, it is reasonable to postulate that forgiveness may also serve as a protective factor in this relationship, decreasing the likelihood that someone with a history of ACEs will develop symptoms of depression. However, it is reasonable to presume that there may be differences when the research is conducted in different countries, especially if they have a different cultural basis, while similar research is limited. Leach and Parazak (2015) have highlighted the importance of assessing the role of culture in a forgiveness study based on the understanding that forgiveness is context-bound, and there is still limited research investigating the dynamics of the association between forgiveness and other variables across the country. Sparse evidence showed that forgiveness has different a meaning, process, and mechanism across culture, mostly comparing individualistic and collectivistic countries. To be sure, a review by Sandage and Williamson (2005) has explained the differences in forgiveness according to its dimensions between individualistic cultures, such as the United States population, which has been widely used in previous studies, and collectivistic cultures, such as the Indonesian population used in this study.
Some of the studies on distress and depression may indicate predictive variation of forgiveness according to its dimensions, which also emphasizes the need for studies in different countries, in this case Indonesia with its collectivistic culture. A study conducted by Gençoğlu et al. (2018) among Turkish university students found that forgiveness of self and situations was negatively associated with depression, anxiety, and stress symptoms, while forgiveness of others was not a significant predictor of depression, anxiety, or stress. This is in line with the results of a study from Poland by Kaleta and Mróz (2020) in which the ability to overcome unforgiveness of oneself and of situations beyond anyone’s control turned out to be significant for the level of depressive symptoms, but not the ability to overcome unforgiveness of others. Furthermore, Gabriels and Strelan (2017) added that in both the Australian undergraduates and North American general sample, relationship-focused forgiveness magnified the distress caused by exploitation risk, whereas self-focused forgiveness, relative to relationship-focused forgiveness, provides a buffer against it. It is important to identify which of the dimensions of forgiveness may be of particular importance in better understanding the relationship between ACEs and depression, both as a mediator and as a moderator.
Considering the relevant involvement of forgiveness in the relationship between ACEs and depression, we hypothesize that forgiveness can be a key factor for mediation analysis. Researchers also conduct mediation and moderation analyses by considering the dimensions of forgiveness. Specifically, we hypothesize that forgiveness in general and by its dimensions (self, others, situations) will mediate the relationship between ACEs and symptoms of depression. We also hypothesize that the dimensions of forgiveness will serve as moderators such that individuals who have high ACE scores but are also high in forgiveness dimensions will have lower depression scores than those with high ACE scores and low scores on these variables. While we will test all forgiveness dimensions in both sets of analyses, significant findings regarding each dimension of forgiveness in previous studies are limited. Therefore, our hypotheses surrounding these two facets are more exploratory in nature.
PARTICIPANTS AND PROCEDURE
PARTICIPANTS
Participants in the present study were 398 students from a university in Semarang, Indonesia who were obtained using cluster random sampling technique of the available faculties. The sample met the minimum recommended number based on the population size in this study’s calculation according to the formula by Krejcie and Morgan (1970). Participants took the first year specifically in the second semester of their education (with an age range from 17 to 21, M = 18.60, SD = 0.60, male = 26.10%). The majority of them represented faculties from the field of Science and Technology (77.39% from the Faculty of Public Health, Science and Mathematics, and Engineering), while the rest were from the field of Social Sciences and Humanities (22.61% from the Faculty of Psychology). A total of 86.68% reported achieving a grade point average (GPA) of at least 3 (out of 4) in their first semester. 44.20% of the entire study sample reported having at least 1 to a maximum of 7 ACEs. The majority of the participants were Javanese (75.17%), so were native to the region where the study was conducted. The detailed demographic characteristics of the participants are presented in Table 1.
Table 1
Demographics of study sample
RESEARCH DESIGN AND PROCEDURE
This research was a cross-sectional study using a quantitative approach. It was conducted in accordance with the ethical standards in the Declaration of Helsinki in 1975 as revised in 2000, in this case by providing a research explanation and written informed consent of each participant. Permits to conduct research on first year students were officially granted to the faculties involved. Data retrieval was through contact with the appointed employee after obtaining approval from the dean of each faculty. The researchers involved assistants in collecting data in the classroom using the paper and pencil test method taken in 2017 before the COVID-19 pandemic.
MEASURES
Demographic characteristics were obtained through written responses containing sex, age, ethnicity, year of study, subject of study and the latest GPA. Measurements were conducted using the Adverse Childhood Experiences (ACEs) questionnaire, the Beck Depression Inventory-II (BDI-II), and the Forgiveness Scale, which are described below.
The Adverse Childhood Experiences (ACEs) Questionnaire by Feliti et al. (1998) was used in this study to measure experiences of childhood adversities. It contains 10 ACEs categorized into three groups, namely childhood abuse (emotional, physical, and sexual), childhood neglect (emotional and physical), and household dysfunction (parental separation, domestic violence, substance abuse, mental illness, and incarceration). The ACEs Questionnaire had been adapted into Indonesian and applied to undergraduates with Cronbach’s α internal reliability of .75 (Kaloeti et al., 2019), while Cronbach’s α in this study was .62, which is still considered weak. The Cronbach’s α estimate was deflated most likely due to the small number of scale points considering its binary responses (Liu et al., 2010). However, the validation of this questionnaire by Feliti et al. (1998) proved that there were strong dose-response relationships between the number of childhood exposures and each of the ten risk factors for the leading causes of death (p < .001), as well as significant dose-response relationships (p < .05) between the number of childhood exposures and some disease conditions. Researchers have also included peer victimization that was bullying and parental death as additional items since they were considered as adversity experiences for childhood (Finkelhor, 2020; Mersky et al., 2017; Murphy et al., 2014). Each type of ACE identified in the first 18 years of life was represented by one item whose response was coded as a binary variable (occurred – 1, absent – 0). Since there was a total of 12 items, the total score of the ACEs ranged from 0 to 12 to obtain the cumulative number of participants’ adversity experiences.
Beck Depression Inventory-II (BDI-II; Beck et al., 1996) was used in this study to measure depressive symptoms. This self-report inventory contained 21 items representing physical, emotional, cognitive, and motivational manifestations. Participants were asked to choose one of four statements in each item that best described themselves and their feelings over the past two weeks. The adaptation of the BDI-II into Indonesian has been carried out previously and tested on the general population with Cronbach’s α internal reliability of .90 (Ginting et al., 2013). Each statement on each item had a score of 0 to 3 indicating absence of the symptom to presence of the severe symptom, so that the total score ranged from 0 to 63. Classification of depressive symptoms included normal indication (scores 0 to 10), mild depression (scores 11 to 16), borderline depression (scores 17 to 20), moderate depression (scores 21 to 30), severe depression (scores 31 to 40), and profound depression (scores above 40). Cronbach’s α in this study was .83.
The Forgiveness Scale used in this study was a Likert scale designed based on Thompson et al. (2005) by paying attention to the three dispositional of forgiveness. A total of 274 college students were involved in the tryout on the Forgiveness Scale by Rahmandani et al. (2016). There were 48 items obtained on the whole scale, 40 items of which measured forgiveness in general, 14 items measured self-forgiveness (positive sample item – “I believe there is still a lot of goodness that I can do to make me feel meaningful”), 19 items measured forgiveness of others (positive sample item – “I can see goodness in others who have hurt me”), and 13 items measured forgiveness of situations (negative sample item – “It is difficult for me to find the good things behind the bad event[s] that befell me”). Cronbach’s α values in this study were .90, .78, .87, and .82, respectively. Since the total items from all subscales were 46, while there were 48 items on the entire scale, the researchers stated that of 48 items there were two items from the forgiveness in general scale that had low item inter-correlations when they were calculated separately based on the subscales, and therefore were not included in the subscales (one each on the forgiveness of self and others subscale). This scale was later used in subsequent studies. Participants were asked to respond to how the item represented themselves, namely with 4 response choices from strongly disagree to strongly agree. The scoring ranged from 0 to 3 on positive items, but from 3 to 0 on negative items. The total score was the sum of the values for all items in each scale/subscale.
ANALYSIS
The analysis phase began with carefully scoring in accordance with the instructions and entering data for processing. Researchers explored the prevalence of demographic characteristics, depressive symptoms and ACEs in participants, as well as interpreting the tendency of forgiveness levels. We then performed prerequisite tests regarding normality and linearity for further analysis. Bivariate correlations were performed to determine whether there were relationships between IV (ACEs), mediator (forgiveness and its dimensions), and DV (depression). Specifically identifying by type of ACEs was also performed as an additional analysis. Path analysis was then performed on the three variables, i.e. ACEs, forgiveness, and depression, with forgiveness as a mediator. Path analyses were also performed to examine the combined and separate effect of the three dimensions as mediators of the relationship between ACEs and depression. Support for the role as mediators was also investigated using confidence intervals (CI), i.e., if the 95% confidence interval of the lower and upper levels in the overall standardized indirect effect did not cross zero. Finally, moderation analyses were conducted in accordance with Hayes (2018) to determine whether any of the forgiveness dimensions significantly moderated the relationship between ACEs and depression. Each dimension of forgiveness was considered a moderator if the interaction term in the analysis was significant. The significance of moderation was analyzed by calculating the effect of ACEs on depression, i.e. regression with moderator value using a cut-off mean ±1 standard deviation. All data analysis was carried out with the help of the software LISREL 9.1 (Student Version) and SPSS Statistics Version 22.
RESULTS
In terms of ACEs’ prevalence in the entire study sample (M = 0.71, SD = 1.09), 55.80% had no experience with ACE until most reported 7 ACEs at 0.50% – the percentage decreased with ACEs (see Table 1). Table 2 shows that 44.20% of the sample experienced at least one ACE, the majority of which (71.60%) were obtained through bullying by external parties. Meanwhile, in the main support system, the highest prevalence of ACEs among survivors was in the category of childhood abuse (39.20%) particularly the emotional type (19.90%) followed by the physical type (15.30%). The prevalence by sex can be seen in Table 2, indicating that females experienced ACEs more, i.e., having experienced ACE(s) 1.79 times in general and 1.38 to 6 times according to its types – except for household dysfunction, and substance abuse, which had the same prevalence (1.1% each among survivors). However, the mean number of ACEs in males was 1.49 times higher than in females. Remaining details of prevalence can be seen in Table 2.
Table 2
Prevalence of childhood exposure to adversity experiences
[i] Note. a ‘Any category reported’ means the sum of participants who reported exposure to at least one adverse childhood experience (ACE). The percentage in ‘any category reported’ was from the entire study sample (N = 398), while the percentage divisor for each type of ACE was ‘any category reported’ (n = 176).b Mean and SD ACEs were the calculation of the entire study sample.
The distribution of depressive symptoms was quite wide with M = 13.07 and SD = 7.00 (see Table 3). Prevalence decreased with increasing symptoms, i.e. 41.71% (n = 166) had normal indications, 30.65% (n = 122) had mild depression, 14.32% (n = 57) had borderline depression, 11.06% (n = 44) had moderate depression, 2.28% (n = 9) had severe depression, and no one had profound depression. Meanwhile, forgiveness and its dimensions tended to be high, as could be seen from the higher mean values and the smaller standard deviation values, for empirical compared with hypothetical values.
Table 3
Correlations among measures
[i] Note. ACEs – adverse childhood experiences. Correlation coefficients between the main variables (ACEs, forgiveness and its dimensions, depression) were the result of the Pearson correlation analysis (assumption tests were fulfilled, in bold), while correlation coefficients containing the types of ACEs (childhood abuse, childhood neglect, household dysfunction, bullying, parental death) were the result of the Spearman’s rho correlation analysis (assumption tests were not fulfilled). *p < .05, **p < .01, ***p < .001.
Bivariate correlations as in Table 3 show that ACEs correlated with depression positively in contrast to forgiveness and its dimensions, which correlated negatively, except for forgiveness of others, which did not correlate. Depression was negatively correlated with forgiveness and all of its dimensions, but the coefficients were much lower for forgiveness of others. Among all types of ACEs, only parental death was correlated with household dysfunction. Bullying was only correlated with childhood abuse and neglect. Household dysfunction and parental death were not correlated with depression. In relation to forgiveness, the types of ACEs that were significantly correlated were only childhood abuse (by dimensions, significant only in forgiveness of situations) and bullying (by dimensions, significant in forgiveness of self and situations). The relationship between the forgiveness dimensions was consistent with previous studies demonstrating that the lowest correlation was between forgiveness of others and self-forgiveness (Rahmandani et al., 2020).
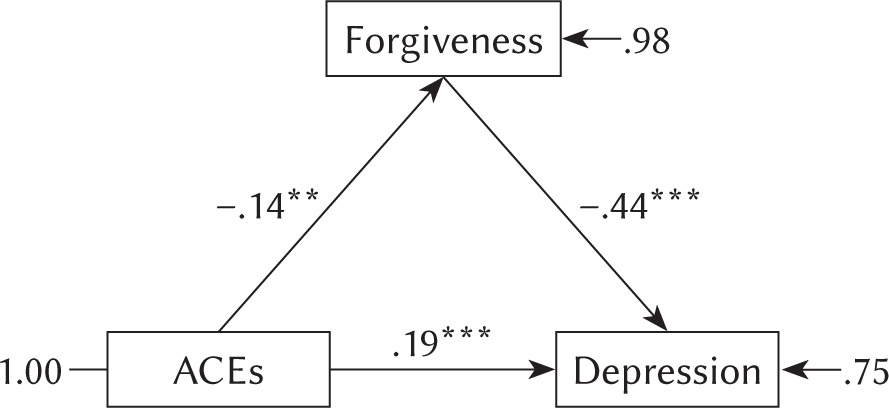
The first model of path analysis was made to examine the mediating effect of forgiveness in general on the relationship between ACEs and depression. Goodness of fit for the model was obtained, with χ2 = 0.00, p = 1.00, and RMSEA = 0.00. Figure 1 shows that ACEs has a direct effect on forgiveness (B = –.17, SE = .06, β = –.14, p = .004) and depression (B = .30, SE = .07, β = .19, p < .001). Forgiveness has a direct effect on depression (B = –.59, SE = .06, β = –.44, p < .001). Forgiveness partially mediates the relationship between ACEs and depression (Sobel’s test on the indirect pathway was significant, with z = 2.32, p = .010). ACEs accounted for 2.04% of the variance in forgiveness and 6.5% of the variance in depression. Both predictors together explained 25.5% of the variance in depression.
Figure 1
The mediation model of forgiveness in the relationship between ACEs and depression
Note. ACEs – adverse childhood experiences. All coefficients in the figure are standardized; **p < .01, ***p < .001.
The second model of path analysis was made to examine whether or not each of the dimensions of forgiveness significantly mediated the relationship between ACEs and depression. The analyses revealed that self-forgiveness and forgiveness of situations were significant mediators in this relationship (see Figure 2). ACEs had a direct effect on self-forgiveness (B = –.10, SE = .04, β = –.14, p = .005) and forgiveness of situations (B = –.11, SE = .04, β = –.13, p = .011), then both self-forgiveness (B = –.66, SE = .08, β = –.34, p < .001) and forgiveness of situations (B = –.56, SE = .07, β = –.32, p < .001) had a direct effect on depression. Meanwhile, only forgiveness of others that was not affected by ACEs (B = –.07, SE = .04, β = –.08, ns) and did not have a direct effect with depression (B = .12, SE = .07, β = .07, ns). Both self-forgiveness (z = 2.77, p = .002) and forgiveness of situations (z = 2.53, p = .005), except forgiveness of others (z = –0.88, ns), partially mediated the relationship between ACEs and depression. All predictors together explained 28.8% of the variance in depression. The standardized confidence intervals of all dimensions for depression are shown in Table 4 and support the explanation why only forgiveness of others did not have a mediating effect significantly, with values of –.02 to .17 that were crossing zero (Hayes, 2018).
Figure 2
The mediation model of forgiveness dimensions in the relationship between ACEs and depression
Note. ACEs – adverse childhood experiences. All coefficients in the figure are standardized; *p < .05, **p < .01, ***p < .001.
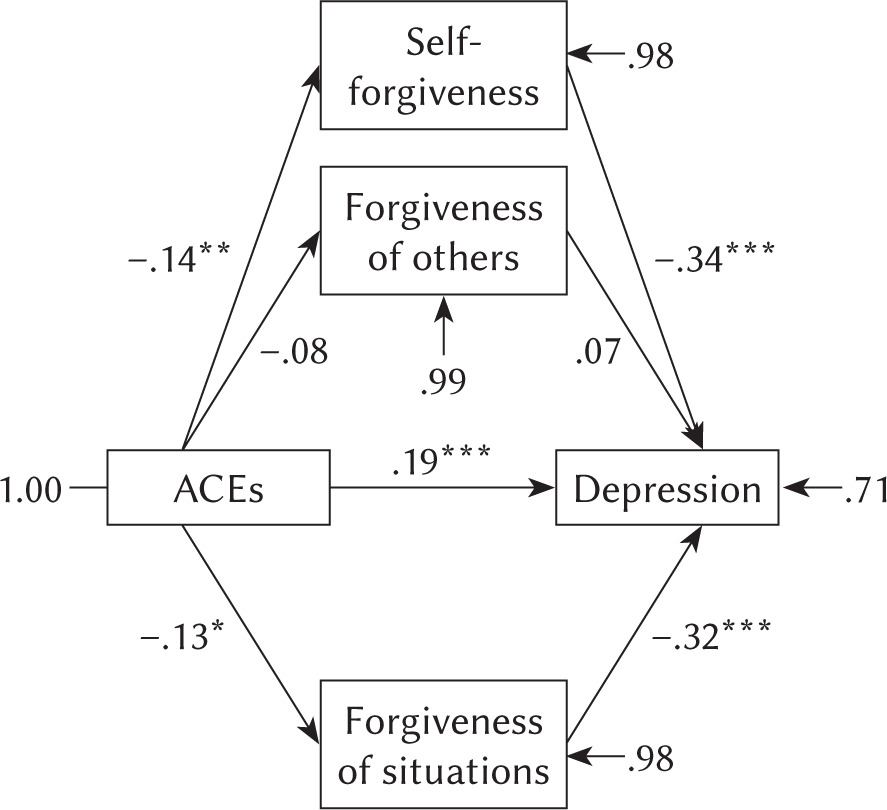
Table 4
The three dimensions’ completely standardized confidence intervals for depression
| Outcome | Forgiveness dimension | Lower CI | Upper CI |
|---|---|---|---|
| Depression | Self | –.45 | –.23 |
| Others | –.02 | .17 | |
| Situations | –.44 | –.19 |
The mediation models of forgiveness dimensions separately were also performed (the figures are not displayed here). Self-forgiveness and forgiveness of situations were clearly mediating. The mediation model of self-forgiveness alone explained 31.90% of the variance in depression, while forgiveness of situations alone explained 29.80% of it. On the other hand, although it was directly related to depression (B = –.27, SE = .08, β = –.15, p = .001), forgiveness of others was not significantly associated with ACEs (B = –.07, SE = .04, β = –.08, ns) and did not mediate ACEs and depression (z = 0.87, ns).
Each of the three dimensions of forgiveness was also analyzed regarding its moderation for the relationship between ACEs and depression (see Table 5). ACEs had a significant main effect in each analysis. There was also a significant main effect of the forgiveness variable for every dimension of forgiveness. Additionally, there was significant interaction for forgiveness of others, indicating that the forgiveness of others significantly moderated the relationship between ACEs and depression. Table 5 lists the main effects and interactions for all variables.
Table 5
Predicting depression by ACEs score, forgiveness dimensions, and their interactions
[i] Note. ACEs – adverse childhood experiences. For each analysis ACEs, the respective forgiveness dimension, and the interaction between those two variables predicted symptoms of depression. Significant variables in the first two columns indicate significant main effects. Moderation was indicated by a significant interaction. *p < .05, ***p < .001.
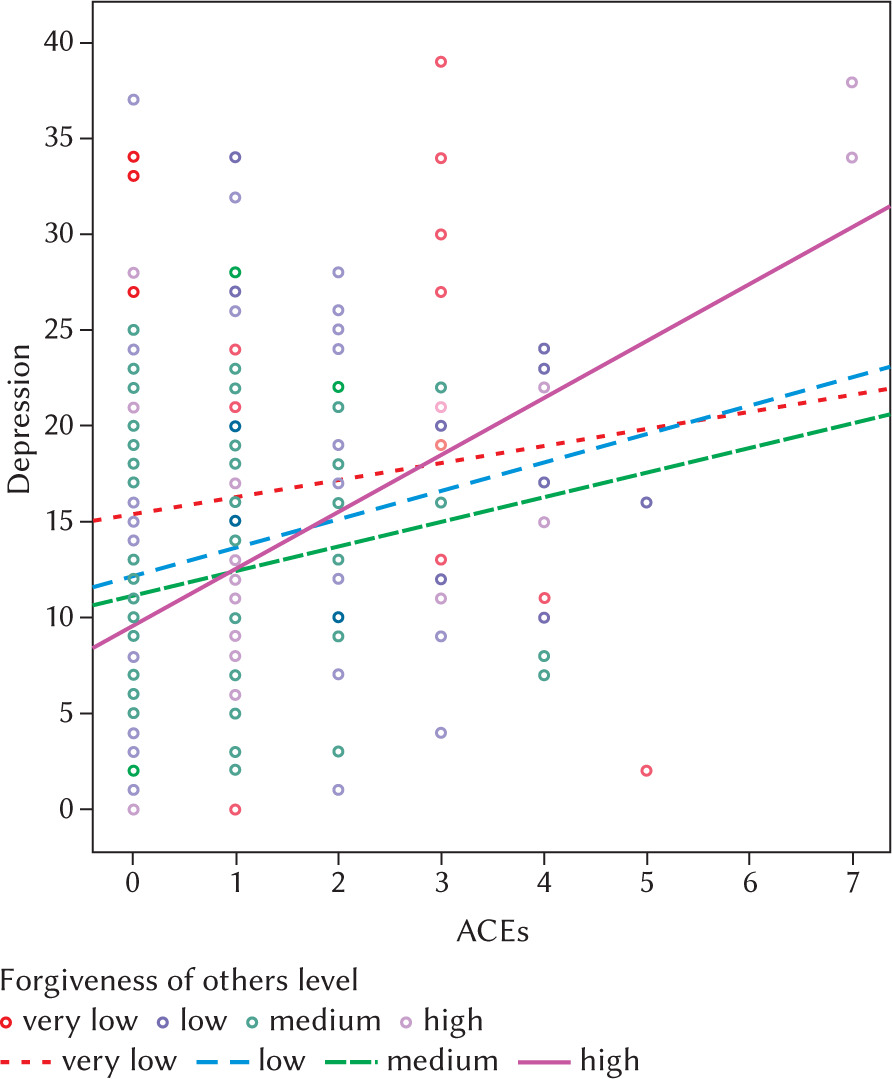
Figure 3 demonstrates the effects of ACEs on depression at very low, low, medium, and high levels of forgiveness of others. According to Hayes (2018), standard values used to determine cut-off scores for low and high levels of forgiveness towards others were one standard deviation below and above the mean score, while the mean score itself was the cut-off score for medium levels. ACEs significantly predicted depression starting from a low (cutoff score of 29.07) to a high (cutoff score of 42.55) level of forgiveness of others. For those with a very low level of forgiveness of others (below the mean by more than one standard deviation), an increase in ACEs was unrelated to an increase in depression scores. Interestingly, the prediction of forgiveness towards others at the medium level was lower than at the low level (R2 was .02 below) but much higher at the high level (R2 was .29 above the medium level). This indicates that an increase in forgiveness of others, or at a high level, was actually a greater predictor of depressive symptomatology as a result of the addition of ACEs. Specifically, those with high levels of forgiving others who did not have ACEs showed lower to normal levels of depression, but levels of depression increased, exceeding those with lower levels of forgiving others even after only one to two ACEs. On the other hand, it predicted little or nothing if the level of forgiveness of others was at a low level or decreasing to a very low level. In short, those who shared more ACEs could have higher depressive symptoms if they had high levels of forgiving others.
Figure 3
The association between ACEs and depression as moderated by forgiveness of others
Note. ACEs – adverse childhood experiences. The categories of forgiveness of others followed the cutoff scores that were low, medium, and high – 29.06, 35.81, and 42.55, respectively. The correlation coefficient (rxy) in each category was very low = .13 (ns, R2 = .02); low = .23** (R2 = .05); medium = .18* (R2 = .03); and high = .57*** (R2 = .32). *p < .05, **p < .01, ***p < .001.
DISCUSSION
Our finding regarding forgiveness as a mediator in the relationship between ACEs and depression was consistent with previous studies. In one study, forgiveness in general was negatively predicted by ACEs whereas depression was positively predicted by ACEs (Crandall et al., 2019). In addition, a study by Arslan (2017) showed that forgiveness in general mediated the relationship between the type of ACEs, i.e. psychological maltreatment, and the mechanism of externalizing maladaptive behavior, i.e. internet addiction. Internet addiction itself has been associated with depression as a risk factor (e.g. Liang et al., 2016).
Specifically, the results of this study emphasized that self-forgiveness mediated the relationship between the two variables with the highest coefficient. Kliethermes et al. (2014) explained that changes in self-perception and overall self-belief about the world happened as a result of ACEs, causing impairment in self-concept (Cook et al., 2005). The low self-concept among those with ACEs resulted in depressive symptoms leading to suicide behavior (Wong et al., 2019). The mechanism in those with low self-concept was that there was negative self-appraisal which became the strongest predictor of suicidality among other predictors (Madsen & Harris, 2021). This condition indicated low levels of self-forgiveness. Self-forgiveness itself involved reducing negative and increasing positive thoughts, emotions, motivations and behaviors regarding oneself (Davis et al., 2015). In collectivist cultures, self-forgiveness was valued low (Sandage & Williamson, 2005), but it was a critical concern since its contribution as a mediator and correlations with both ACEs and depression were highest among the other dimensions. When self-forgiveness was low as a result of more ACEs, then self-coldness increased, resulting in self-criticism tendencies and negative emotional symptoms would lead to psychological vulnerability (Megawati et al., 2018). When self-critical persons perceived failure, they would criticize themselves in a hostile manner, generate feelings of worthlessness, and perpetuate negative affect.
Previous research explaining the mediating effect of forgiveness of situations in this context was limited. We postulated that forgiveness of situations might be a significant mediator in the relationship between ACEs and depression due to the fact that the nature of adversity experiences – even if it was done by another person and not as a result of disasters – was an event beyond the child’s control. This is in line with the definition of forgiveness of situations (Lopez et al., 2015). On the other hand, blaming others was a wrong idea because their presence was ‘socially acceptable’ especially if the perpetrator was a person within the family, such as a caregiver or who was supposed to be a protector and attachment figure (Santrock, 2014). Of course, the presence of events in collectivistic culture was also determined. Adversity experiences beyond the child’s control were reasonable because children were powerless and less educated. A high number of ACEs might harm a child’s ability to control the situations effectively. On the other hand, children lost support for mastery of affective and behavioral regulation, good appraisal, decision making and adaptive coping, which ultimately resulted in difficulties in overall psychological areas throughout the lifespan (Lawson & Quinn, 2013). Lower forgiveness of situations due to more ACEs resulted in higher feelings of threat in the midst of high stressful situations, potentially causing feelings of hopelessness, defeat, and entrapment, resulting in depression and suicidal behavior (Panagioti et al., 2012).
Our finding that forgiveness of others did not mediate other moderators as a risk factor could also be explained. Those results might contradict a previous systematic review of studies involving participants with experience of man-made trauma which explained that the majority of studies reviewed found a significant correlation between forgiveness of others and symptomatology that was post-traumatic stress disorder (PTSD) (Cerci & Colucci, 2018). However, there was a study supporting the current result that forgiveness of others in victims of man-made trauma was not associated with PTSD symptoms. Those reviews also emphasized that there were factors that influenced the results, one of which was a culturally sensitive context. Previous studies explained how forgiveness of others worked in collectivistic cultures. Globally, forgiveness of others involves other-focused concerns. It is more intended for interpersonal functioning and obtaining a sense of social harmony (Enright et al., 1998; McCullough & Witvliet, 2002). Forgiveness in collectivistic cultures includes societally enforced ideals or strong norms to maintain social harmony (Karremans et al., 2011; Sandage & Williamson, 2005) even if one is not ready to reconcile (Hook et al., 2012) or it causes more self-sacrifice (Akhtar, 2013). That reason also explained why the correlation coefficient between forgiveness of others and self-forgiveness was the smallest but self-forgiveness contributed the most to ACEs and depression, consistent with previous studies (e.g. Rahmandani et al., 2020). Ignorance or low levels of forgiveness of others, in contrast to increased self-concern, might be a mechanism for detaching oneself from the experience of transgression and gaining a sense of peace from unforgiving others (Jones Ross et al., 2017), instead of forcing compliance with collective norms so as to attenuate the occurrence of depressive symptoms due to other-related transgression. Under different conditions, the addition of ACEs will result in greater emotional distress in those with high forgiveness of others, thereby rapidly increasing depressive symptoms.
Regardless of the culture-related explanation, however, the trend of the relationship between the forgiveness dimensions and depression has been typically found in studies in east and west bordering countries such as Turkey (Gençoğlu et al., 2018) or Poland (Kaleta & Mróz, 2020), namely that forgiveness of self and situations was associated with depression, but not forgiveness of others. A study involving patients from a clinic in the southeastern United States also confirmed that the relationship between adversity experience, i.e. domestic abuse and a mental health symptom, i.e. suicide behavior, was accounted for by forgiveness of self, but not by forgiveness of others (Chang et al., 2014). This implied differences in influence that were more extensive than those limited to collectivistic cultures. A study that targets these two different cultures could be a possibility for further research.
The results of this current study also indicated the contribution of different types of ACEs. The current study showed that forgiveness in general was negatively correlated with a specific type of ACEs that was abuse-related childhood adversity, i.e. childhood abuse in the family, and peer-related abuse or peer victimization, in this case bullying. According to the dimensions, childhood abuse in the family was specifically correlated with situations forgiveness, while bullying was specifically correlated with self and situations forgiveness. The forgiveness of others was not correlated with either of those two other-related transgressions. All forgiveness dimensions were correlated with depression – the forgiveness of others was the lowest. In addition to the discussion before, these results both contradicted and supported a narrative review by Sinclair et al. (2020) which explained that positivity could be misdirected or overgeneralized thus exacerbating harm and abuse and increasing the likelihood of further transgressions, for example due to refraining from leaving abusive relationships. Another study explained that general interpersonal distress and several specific areas of interpersonal problems in adulthood were significantly associated with childhood experiences, in this case emotional abuse, emotional neglect, and sexual abuse (Huh et al., 2014). The contradiction to the review by Sinclair et al. (2020) can be seen in the current study, where positivity in the form of self-forgiveness and forgiveness of situations decreased due to an increase in ACEs, thereby increasing symptoms of depression. On the other hand, support can be seen in the possibility that participants might maintain forgiveness of others at higher levels (as well as at lower levels, indicated by the absence of its association with ACEs and CI crossing zero) even though it finally led to greater depression. These explanations eventually also answer how the collectivistic culture distinguished forgiveness according to its dimensions in terms of mediation and moderation.
From the discussion above, the results of this study explained how collectivistic cultures were likely to respond to different contributions in mediation and moderation. The nature of others forgiveness that was put forward because of social harmony made it unrelated to ACEs and did not mediate the relationship between ACEs and depression especially if it was an abuse-related childhood adversity as in this study; on the contrary, it moderated it as a risk factor. In addition, self-forgiveness was not valued but greatly contributed to mediation – at least self-concern offered detachment from the experience of transgression, instead of forcing compliance with collective norms. Situations forgiveness took on a mediating role because it was beyond the child’s control during the adversity experience. However, we also considered the possibility of different influences that were more extensive than those limited to collectivistic cultures.
Limitations to our study included a limited incidence of ACEs among the general college student population and consideration of demographic variables. Although our sample was representative of the incidence in the college student population in general, this study might not represent how these dynamics of mediation and moderation occurred in those with ACEs or those receiving mental health services as its result. We also did not use our demographic variables as controls or conduct separate analyses to determine whether our results would differ for different demographic groups, such as in terms of sex and culture. Although our sample represented a country from collectivistic cultures, ethnic diversity needs to be taken into consideration considering that Indonesia is an archipelagic country.
This study is expected to increase practitioners’ understanding of the incidence of depression as a result of ACEs through forgiveness, as well as to be a consideration in planning and providing interventions. Future research may wish to consider involving specific populations of students, such as users of mental health services or those who have been identified as having experienced certain types of trauma, as well as determining whether these effects will hold in demographically different groups, such as paying attention to sex and ethnic differences. A study that targets both different collective and individual cultures can be designed for further research. Finally, since this study was conducted in the field of education, the future study is also suggested to involve academic-related variables to gain more understanding regarding the impacts of the three variables on academic processes and outcomes, such as students’ behaviors and their academic achievements.
CONCLUSIONS
The purpose of this study was to explore the decreased forgiveness and its dimensions as a mechanism in individuals with a history of ACEs who might develop depressive symptomatology, as well as to identify the dimensions of forgiveness as potential factors in the relationship between those two variables. This study found that forgiveness in general and its dimensions, particularly self and situations forgiveness, significantly mediated the relationship between ACEs and depression. The higher number of ACEs resulted in lower levels of forgiveness, which in turn increased depression. We also found that forgiveness of others, which did not mediate, moderated (and only forgiveness of others) the relationship but as a risk factor. This means that high levels of forgiveness of others will increase depressive symptoms when having more ACEs. The increase in depression with the increasing the number of ACEs slowed down and forgiveness of others was lower.