BACKGROUND
Survivors of intensive care units (ICUs) face several somatic and psychological challenges. Systematic reviews show that the prevalence of post-traumatic stress disorder (PTSD) symptoms varies between 11% and 21% (Righy et al., 2019) among ICU survivors three months after the ICU stay. Also, two to three months after an ICU stay, the prevalence of anxiety and depressive symptoms varies between 22% and 38% (Nikayin et al., 2016; Rabiee et al., 2016). In addition, former ICU patients report a deterioration in health-related quality of life (HRQoL), compared to that before the ICU stay (Dowdy et al., 2005), a drop that has been linked to PTSD (Davydow et al., 2008), anxiety (Nikayin et al., 2016), and depressive symptoms (Rabiee et al., 2016). The somatic HRQoL is most affected during the first three (Cuthbertson et al., 2010) to six months (Fildissis et al., 2007), followed by a slow improvement in the HRQoL about two years after the ICU stay. The above findings highlight the importance of identifying factors that could predict which individuals are at high risk of developing distress symptoms.
At two to three months follow-ups after the ICU discharge, prior psychiatric history has been linked to the appearance of PTSD, depressive, and anxiety symptoms (Samuelson et al., 2007; Schandl et al., 2013; Wade et al., 2012). Also, unemployment or protracted sick leave and lower socio-economic status (SES) were related to anxiety and depressive symptoms (Schandl et al., 2013; Wade et al., 2012). Furthermore, chronic physical health problems have been linked to anxiety symptoms (Wade et al., 2012). Finally, regardless of assessment time after the ICU stay, PTSD symptoms have been linked inconsistently to female gender (for a review see Wade et al., 2013; Parker et al., 2015) and anxiety symptoms have been linked inconsistently to low educational levels (Nikayin et al., 2016).
Concerning medical factors, illness severity at admission to the ICU and length of stay in the ICU are unrelated to PTSD, anxiety, and depressive symptoms (McGiffin et al., 2016; Wade et al., 2013), but mechanical ventilation (MV) related variables, such as length of time, or sedation and analgesia practices have been inconsistently related to PTSD symptoms (McGiffin et al., 2016; Parker et al., 2015). It has been suggested that agitation, physical restraint, and administering sedating and/or analgesic medications, during the ICU stay, are all positively related to acute stress symptoms following an ICU discharge (Jackson et al., 2016). Limited findings suggest that delirium in the ICU is in turn related to anxiety (Nikayin et al., 2016) and depressive symptoms (Rabiee et al., 2016).
Emotional stress reaction in the ICU, the subjective perception of the total ICU experience as a negative one, and negative ICU memories have been linked to the occurrence of PTSD, depressive, and anxiety symptoms at two- to three-month follow-ups after the ICU discharge (Samuelson et al., 2007; Schandl et al., 2013; Wade et al., 2012). In addition, feelings of helplessness in the ICU (assessed in the hospital up to four weeks following ICU discharge) have been linked to depressive symptoms at six months after the ICU stay (Wintermann et al., 2018). Finally, being confused about what happened in the ICU has been linked to PTSD symptoms (Wade et al., 2013). Therefore, the way former patients handle ICU memories and make sense of the ICU experience, especially soon after the ICU discharge, may be an important factor for the experience of psychological morbidity later.
Following a traumatic event, individuals try to process and understand the experience over time using various means, one of which is the opportunity to discuss the event with their social network (Ehlers & Clark, 2000). According to Lepore (2001), discussing a traumatic experience with supportive/receptive others may assist individuals to reflect on and process trauma-related thoughts and feelings, organize traumatic memories and increase control over negative emotional responses (Lepore, 2001). In contrast, when individuals believe or feel that their social environment is negative or unsupportive to that kind of disclosure (social constraint), they tend to avoid discussing the traumatic experience, thus limiting the opportunity to further process the experience (Lepore, 2001). In addition, former patients may interpret the reluctance of their relatives to get involved in conversations regarding the ICU stay as an indication that their social environment would not effectively support them and thus they may experience feelings of frustration and anxiety (Rini & Schetter, 2010).
The present study was based on a sample of Greek patients assessed approximately three months after they were discharged from the ICU. The main goals of the study were to 1) report the frequency and severity of psychological morbidity (PTSD, anxiety, and depressive symptoms) and HRQoL status and 2) report the correlates (demographic, psychosocial, ICU negative memories, and medical factors) of psychological morbidity. In addition, the main goal of the study was to test the hypotheses that 1) HRQoL would be negatively related to psychological morbidity and 2) the social constraint (SC) that patients experienced when they talked about their ICU stay would be a predictor of psychological morbidity three months after discharge.
PARTICIPANTS AND PROCEDURE
PARTICIPANTS
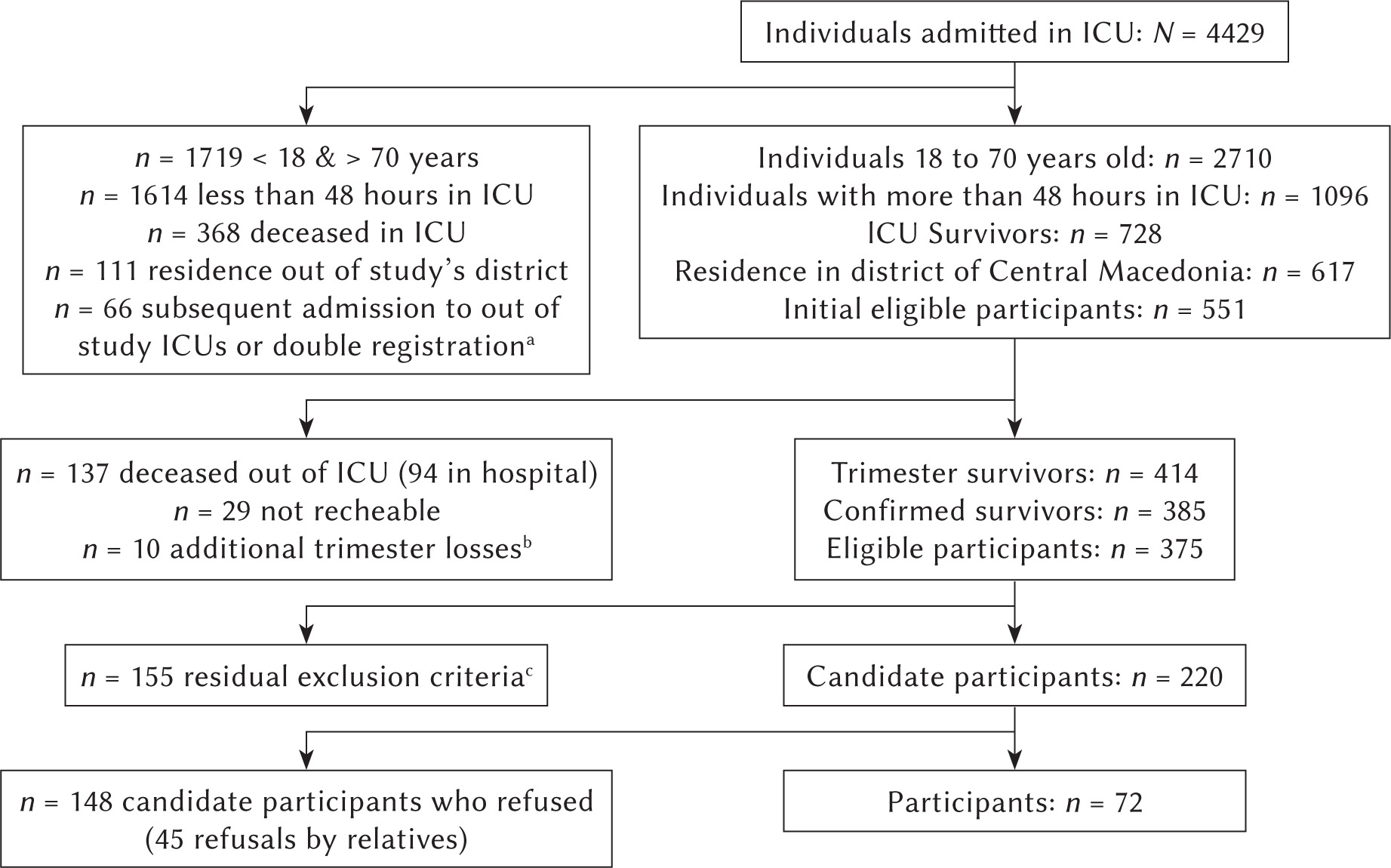
Study participants were patients admitted to the ICU of five hospitals in Thessaloniki. For each hospital, the study was approved by the scientific committee and the hospital board (Ippokratio General Hospital (GH), Ref.: 654/08.07.2015; Agios Pavlos GH, Ref.: 32th session/Γ11/31.12.2015; Agios Dimitrios GH, Ref.: Δ3β/10902/05.04.2016; Theagenio Cancer Hospital, Ref.: 15804/20.05.2016; G. Papanikolaou GH, Ref.: Δ3β/20567/30.06.2016). In total, 4429 patients were admitted to the study’s ICUs between August 2015 and August 2018 and were consecutively screened for inclusion (Figure 1). Stepwise inclusion criteria were: age between 18 and 70, at least 48 hours in the ICU, survival, and permanent residence in the district of Central Macedonia. The following exclusion criteria were applied to the remaining 375 eligible participants: 1) suicide attempt (admission diagnosis), 2) psychotic disorder and/or substance abuse, 3) inability to read and write in Greek based on their own or their relatives’ statement, 4) pending court case, 5) MV less than 24 hours while in the ICU, 6) hospitalization in rehabilitation or other clinics four months after the ICU stay. Of the 220 potential participants, 72 met selection criteria and agreed to participate. The data presented here are the baseline data collected for a larger study.
Figure 1
Flow diagram for study participants
Note. ICU – intensive care unit
aIndividuals (n = 50) who did not survive a second or third admission to an ICU of the study. bFour individuals moved to an area outside the district of Central Macedonia, three individuals were admitted to ICUs not participating in the study and three individuals had difficulty communicating and understanding the study’s procedures. cResidual exclusion criteria: 1) suicide attempt (n = 9), 2) psychotic disorder and/or substance abuse (n = 31), 3) inability to read and write in Greek based on their own or their relatives’ statement (n = 53), 4) pending court case (n = 2), 5) mechanical ventilation less than 24 hours while in the ICU (n = 29), 6) hospitalization in a rehabilitation or other clinic for a period longer than four months (in case of hospitalization at three months, a second attempt of communication was made 15 days later and if hospitalization continued, a last attempt was made at about four months) after the ICU stay (n = 31)
The mean age was 50.49 years (SD = 13.21). Fifty-four (75%) of the participants were married or in intimate relationships. Thirty-four (48%) participants reported low, 36 (51%) medium, and one participant (1%) high income. For statistical purposes, the income variable was recoded into a binary form wherein 34 (49%) participants had low income and 37 (51%) participants had a medium or high income. Twenty-nine (29%) participants had completed six to nine years of school (low level), 33 (46%) had completed 12 years (medium level) and 18 (25%) had a university degree (high level). Before ICU admission, 46 (64%) participants had been working, 10 (14%) had been unemployed and 16 (22%) had been retired. Three months after the ICU stay, the number of retired participants was the same and one (10%) of the initially unemployed participants was employed. However, from the initially employed participants, 22 (48%) stopped working, a significant drop, McNemar-Bowker test of symmetry (3, N = 72) = 19.174, p < .001. Additional demographic information is presented in Table 1.
Table 1
Pearson’s correlations between demographics, psychosocial factors, quality of life and psychological symptoms
[i] Note. N = 72 unless otherwise noted. ICU – intensive care unit; IES-r – Impact of Event Scale-revised; HAS – anxiety subscale of the Hospital Anxiety and Depression Scale (HADS); HDS – depression subscale of HADS; PHCS – psychological health care services; NA – not applicable; EQ – EuroQoL; VAS – visual analogue scale. aA recoded variable where medium values include a participant who reported high income; bnine (69%) cases referred to medical problems and their effects after the ICU stay; caccording to medical files; dthe Spearman statistic was used (three categories or an item with response on a Likert type scale). *p < .05, **p < .01, ***p < .001, °p = .50, °°p = .058.
PROCEDURE
Relatives were contacted about three months after patients’ last ICU stay and a meeting was arranged at the patient’s residence or office (M = 99.18 days, SD = 9.88). During the meeting, participants were informed about the study and signed a consent form which included approval to access their medical files. Then, they completed the study questionnaire. Data were collected between December 11th, 2015, and December 4th, 2018.
MEASURES
The research questionnaire comprised two sections. The first section included demographics, mental health care services (before and after the ICU stay, sessions with a neurologist, when followed by a psychotropic drug prescription, were also classified as mental health care services), and information about any important events (stressors) that might have happened during the time following the ICU stay. The second section consisted of questionnaires assessing ICU negative memories, PTSD symptoms, depressive symptoms, anxiety symptoms, HRQoL, and social constraint (SC).
Negative ICU memories. Four statements were used to assess the existence (yes or no) of the most common negative ICU-related types of memories (nightmares, anxiety, pain, and difficulty in breathing) (Stoll et al., 1999). In the present study, the sum of negative ICU memories (NIM) had acceptable internal reliability (Cronbach’s α = .60) for research purposes.
Stressor-specific distress. Stressor-specific distress was assessed using the Greek version of the Impact of Event Scale-Revised (IES-r; Mystakidou et al., 2007; Weiss & Marmar, 1997). In the present study, the questions (22 items) were asked concerning events experienced during the ICU stay. In ICU survivors, the threshold for individuals to be considered as having substantial or severe PTSD symptoms (from now on referred to as cases) is 36 (or M > 1.6 per item) (Bienvenu et al., 2013). In the present study, Cronbach’s α for the scale was .89.
Anxiety and depressive symptoms. Anxiety and depressive symptoms were measured using the Greek version of the Hospital Anxiety and Depression Scale (HADS; Michopoulos et al., 2008; Zigmond & Snaith, 1983). According to the authors of the scale, the threshold for individuals with at least mild anxiety or depressive symptoms (from now on referred to as cases) is eight (Zigmond & Snaith, 1983). In the present study, Cronbach’s α was .82 and .80, for the anxiety (HAS) and depression (HDS) subscales respectively.
Health-related quality of life. HRQoL was measured using the EuroQoL-5D-5L (EQ) (EuroQol Group, 1990) adapted to the Greek population by Yfantopoulos (2001). The EQ consists of two parts. The first part consists of five items (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), wherein individuals are asked to report the intensity of their problems in each domain. The second part consists of a vertical 0 to 100 Visual Analog Scale (VAS) with 0 and 100 representing the worst and best imaginable health state, respectively, as of today.
Social constraint. SC was measured using the five questions of Lepore’s Social Constraints Scale in Past Week (Lepore et al., 1996) which were translated into Greek and adapted for the ICU population by the researchers. Participants were asked to respond if there were negative feelings and if they experienced difficulty in their conversations about their ICU stay with members of their social network, during the past three months. In the present study, Cronbach’s α for the scale was.70.
MEDICAL DATA
The length of stay in ICU was recorded in days. Mean dosages of midazolam (the only sedative benzodiazepine in the study), fentanyl, remifentanil, and corticosteroids (hydrocortisone equivalents) were recorded in mg. The mean dosage of propofol was recorded in ml of 2% solution. For all medications and MV, duration was calculated as the percentage of days of administration out of total days in the ICU. Also, the duration of the combined fentanyl and remifentanil (opiates) administration was calculated. Participants were registered as positive cases for confusion or delirium (yes or no event) when it was explicitly recorded by ICU physicians as occurring at least once. The Glasgow Coma Scale (GCS) scores near admission were used to assess the level of consciousness upon arrival (scores of 3 indicate deep unconsciousness and scores of 15 indicate a fully awake patient). As 63 (86%) participants were admitted intubated, GCS scores referred to the patient’s consciousness before the intubation. Twenty-six (36%) of the participants who were admitted to the ICU after elective surgery registered as GCS 15. The Acute Physiology and Chronic Health Evaluation II (APACHE II) scores on admission day were used to estimate illness severity. Finally, MV status was assessed using a three-level scale. A high level refers to situations wherein the ventilator was required for breathing (volume control, pressure control). A medium level refers to partial support (pressure support ventilation, synchronized intermittent mandatory ventilation – pressure support, continuous positive airway pressure). A low level refers to all other forms of support provided for the patient’s respiration (T-piece, face mask). We estimated the intensity of weaning based on the number of times the participant’s ventilator was shifted from a lower MV level to a higher one (weaning relapses).
RESULTS
PSYCHOLOGICAL MORBIDITY AND HRQOL STATUS AFTER ICU STAY
Psychological morbidity. Eight (11%, 95% CI [4%, 19%]) participants had IES-r scores higher than 35 (PTSD cases), 26 (36%, 95% CI [25%, 47%]) participants had HAS scores higher than 7 (anxiety cases) and 23 (32%, 95% CI [21%, 43%]) participants had HDS scores higher than 7 (depression cases). Seventeen (65%) of the anxiety cases were also depression cases. Six (75%) of the PTSD cases were also depression cases and five (63%) were also anxiety cases. In total, 34 (47%) participants could be classified as cases of at least one of the above diagnostic categories.
HRQoL status. The EQ frequencies were categorized into four groups, based on the intensity of their difficulties. For each group, we also calculated the VAS values. The group with serious problems consisted of 28 participants (39%) who reported that they had serious difficulties or that they could not execute the specific activity described in at least one area assessed by the EQ (MVAS = 58.39, SDVAS = 19.74). Likewise, 22 participants (31%) reported that they had moderate problems (MVAS = 65.14, SDVAS = 17.35), 18 participants (25%) that they had limited problems (MVAS = 84.67, SDVAS = 15.89) and four participants (6%) that they did not have any problem at all (MVAS = 92.50, SDVAS = 11.90).
RELATIONSHIP BETWEEN DEMOGRAPHICS, NEGATIVE ICU MEMORIES, MEDICAL FACTORS, PSYCHOSOCIAL FACTORS AND HRQOL, AND PSYCHOLOGICAL MORBIDITY
Demographics. Pearson’s correlations or Spearman statistics between demographics and psychological morbidity are summarized in Table 1. Other stressors experienced during the three months after the ICU stay were related to PTSD, anxiety, and depressive symptoms while educational level related negatively to all types of psychological symptoms. PTSD symptoms were also related to female gender and the presence of psychological problems before ICU admission. Anxiety symptoms were also negatively related to income.
Negative ICU memories and medical factors. The results are summarized in Table 2. PTSD symptoms were related to NIM and anxiety ICU memories while anxiety symptoms were related to anxiety ICU memories. PTSD symptoms were related to GCS and mean daily dose of haloperidol. Anxiety symptoms were positively related to GCS and negatively related to the duration of opiate administration. Finally, depressive symptoms were related to weaning relapses and negatively related to the time spent in the ICU until the beginning of weaning as a percentage of the total time spent in the ICU – the later the beginning of weaning, the fewer the depressive symptoms. Depressive symptoms were also negatively related to the duration of opiate administration and mean daily dose of remifentanil.
Table 2
Relations between negative ICU memories and medical factors with psychological symptoms
[i] Note. N = 72. ICU – intensive care unit; IES-r – Impact of Event Scale-revised; HAS – anxiety subscale of the Hospital Anxiety and Depression Scale (HADS); HDS – depression subscale of HADS; APACHE – acute physiology and chronic health evaluation; GCS – Glasgow Coma Scale; MV – mechanical ventilation; NIM – negative ICU memories. aDays in ICU until the beginning of weaning to total days in ICU; bhigher scores refer to more frequent alterations on MV status; cto total days in ICU. *p < .05, **p < .01, ***p < .001, °p = .52, °°p = .056.
Psychosocial factors and HRQoL. The results are summarized in Table 1. SC was related to PTSD, anxiety, and depressive symptoms. The VAS score was negatively related to psychological morbidity and depressive symptoms were related to all the aspects of quality of life. Finally, PTSD and anxiety symptoms were positively related to all aspects of quality of life EQ items except for the one assessing mobility.
PREDICTING PSYCHOLOGICAL MORBIDITY THREE MONTHS AFTER THE ICU STAY
Predicting PTSD symptoms. A stepwise regression analysis was performed with IES-r as the dependent variable and the seven factors that correlated with PTSD symptoms in bivariate analyses (NIM, SC, gender, psychological health care services before the ICU stay, GCS, mean daily dose of haloperidol, and the existence of another stressor) as the independent variables. When the independent variables were conceptually related, only one of them was included in the model. Such variables were anxiety recollections, a component of NIM, r = .75 , p < .001, and a history of psychological problems (medical files) about participants who reported that they had received psychological health care services before the ICU stay, r = .65 , p < .001. The final model consisted of four predictors, NIM, SC, gender (female) and mean daily haloperidol dosage, explaining 33% of IES-r variance F(4, 67) = 9.76, p < .001 (Table 3).
Table 3
Stepwise regression analysis of PTSD symptoms in study participants
Predicting anxiety symptoms. A stepwise regression analysis was performed with HAS as the dependent variable and the six factors related to anxiety symptoms in bivariate analyses (SC, anxiety recollections from the ICU stay, the existence of another stressor, income, duration of opiates administration, and GCS) as the independent variables. The final model included three predictors, SC, the reporting of another stressor, and income, explaining 34% of HAS variance, F(3, 67) = 12.96, p < .001 (Table 4).
Table 4
Stepwise regression analysis of anxiety symptoms in study participants
Predicting depressive symptoms. A stepwise regression analysis was performed with HDS as the dependent variable and the six factors related to depressive symptoms in bivariate analyses (SC, the existence of another stressor, duration of opiates administration, mean daily remifentanil dose, weaning relapses, and time in ICU until the beginning of weaning) as the independent variables. The final model included three predictors, SC, mean daily remifentanil dose, and the existence of another stressor, that explained 27% of HDS variance, F(3, 68) = 9.65, p < .001 (Table 5).
Table 5
Stepwise regression analysis of depressive symptoms in study participants
DISCUSSION
In this retrospective study, we found that almost half of the ICU patients suffer considerable psychological distress three months after being discharged. In addition, we confirmed the hypothesis that health-related quality of life is negatively related to psychological morbidity and that SC predicts psychological morbidity three months after the ICU stay. Specifically, participants were more likely to meet the threshold for anxiety and depressive cases (36% and 32%, respectively) but less likely to meet the threshold for PTSD cases (11%). The case rates were consistent with the international literature, although for anxiety and depressive cases the rates approached the upper bounds of the existing literature, that is 38% for the prevalence of anxiety (Nikayin et al., 2016) and 36% for depressive symptoms (Rabiee et al., 2016), respectively. In contrast, for PTSD cases the rates approached the lower bounds of the existing literature, which were 11% for the prevalence of PTSD symptoms (Righy et al., 2019). Demographic, psychosocial, and medical variables were predictors of psychological distress.
As expected, participants’ HRQoL was worse than that of the general Greek population as only 6% of the participants reported that they had no problems or difficulties, compared to 43% amongst the general Greek population (Kontodimopoulos et al., 2008). Furthermore, aspects of quality of life (e.g., ability to care for one’s self or to engage in everyday activities) were related to the three types of psychological symptoms, the only exception being difficulties in mobility, which was related only to depressive symptoms (Davydow et al., 2008; Nikayin et al., 2016; Rabiee et al., 2016). The strong relationship between psychological morbidity and all aspects of HRQoL is consistent with the observation that HRQoL is most affected during the first three (Cuthbertson et al., 2010) to six months (Fildissis et al., 2007) following the discharge from the ICU. During that time physical difficulties may be a strong contributor to quality of life (Cuthbertson et al., 2010; Fildissis et al., 2007). Similarly, the subjective perception of one’s overall health (VAS), somatic and mental, was related to psychological morbidity, mostly to depressive symptoms. This is consistent with the existing literature, which shows that real or perceived deficits in everyday functioning are linked to higher levels of depression and anxiety among ICU survivors (Abraham et al., 2014), as they are more likely to experience helplessness and strain.
Bivariate analyses showed that psychological morbidity after the ICU stay was related to several demographic factors. Specifically, female gender was related to PTSD symptoms. This finding is in agreement with another study with Greek patients three months after the ICU stay (Asimakopoulou & Madianos, 2014), and with the broader literature on PTSD, which shows that females are two to three times more likely to develop PTSD after a traumatic event due to both psychosocial and biological factors (Olff, 2017). However, it is inconsistent with the majority of the international ICU studies, which indicate that female gender is not related to PTSD symptoms (Parker et al., 2015). The findings regarding gender differences need to be replicated and explored further. In addition, our results showed that some SES variables (i.e. low income, unemployment, and low education level) were related to psychological morbidity, a finding consistent with the international literature (Schandl et al., 2013; Wade et al., 2012). A serious health problem usually results in a loss of resources, a strain compounded by the lack of employment and/or protracted sick leave (Hobfoll, 1989). SES-related variables may be particularly important for our sample given that only one participant reported high income and this study was conducted during the Greek financial crisis of 2008-2018. According to Hobfoll (2002), individuals who possess more recourses are more efficient in dealing with stressful conditions and less vulnerable to circumstantial loss of resources due to stressful conditions. Education, income, and employment are such resources, the lack of which may make it more difficult to cope with ICU-related stressors.
We also found that experiencing other stressors (69% of reported stressors were medical) after the ICU stay was related to all three types of psychological symptoms. Health problems burden former patients, thus inflicting additional stress (Hobfoll, 1989). PTSD symptoms following a medical illness often revolve around the threat that the medical condition will reoccur and/or the patient’s level of functioning will decline in the future (Jackson et al., 2016), both of which are more likely to occur if the person faces additional health threats. Therefore, adverse life experiences after the ICU stay, related or unrelated to the ICU stay, appear to take a toll. Finally, prior psychiatric history was related to PTSD symptoms but not to anxiety and depressive symptoms, a finding partially consistent with the international literature (Parker et al., 2015; Wade et al., 2012). A possible explanation for the lack of effects for anxiety and depression may be the low rate of participants with psychiatric history (13%) combined with the relatively small sample size of this study.
Regarding the impact of medical factors on psychological morbidity, we found that the longer the administration of opiates (analgesia) was, the lower was the prevalence of depressive and anxiety symptoms. The administration of analgesics could, in part, reflect the clinicians’ ways of managing participants’ anxiety, agitation, or pain during the ICU stay (Davydow et al., 2008). The findings also showed that the higher the daily dose of haloperidol was, the more severe were the PTSD symptoms. The administration of haloperidol, an antipsychotic drug, could reflect, in part, the clinicians’ attempts to control intense symptoms of agitation or delirium in the ICU, both of which are related to PTSD or acute stress symptoms after the ICU stay (Jackson et al., 2016). Both of these findings need to be replicated and researched further. Finally, the degree to which patients were aware of the ICU admission procedures and the difficulty of weaning were found to be positively related to psychological morbidity. These variables may reflect the degree to which patients are exposed to potentially adverse conditions during the ICU stay, leading to psychological morbidity. Consistent with the literature, negative memories of the ICU stay predicted PTSD symptoms (Parker et al., 2015). This is an important variable given that 57% of participants reported at least one negative ICU memory.
Most importantly, we found that SC on conversations about the patient’s ICU experience is positively related to psychological morbidity. This finding is consistent with Lepore’s model (Lepore, 2001) and with research findings showing that PTSD symptoms are associated with SC (Widows et al., 2000). It may be that when ICU survivors feel that others are not emotionally available to hear their story, the opportunity to process their experience is restricted, thus leading to more intrusive thoughts about these experiences (Rimé, 1995) and a higher level of PTSD symptoms (Ehlers & Clark, 2000). Ehlers and Clark (2000) suggested that intrusive re-experiencing of traumatic memories could be diminished if the memories are elaborated and integrated into the context of personal experience. Participants who are deprived by their social environment of the opportunity to discuss ICU topics would be less likely to assimilate their memories in an autobiographical context. Indeed, filling memory gaps, forming a personal story, and facilitating communication between former patients and their relatives/caregivers are important goals of interventions based on ΙCU diaries (Egerod et al., 2011; Garrouste-Orgeas et al., 2012). In addition, ICU survivors may feel rejected and a burden to their caregivers when they encounter the reluctance of their family and friends to hear about their ICU experiences, thus increasing the probability of depression (Rini & Schetter, 2010). SC has been related to depression (Cohee et al., 2017; Lepore et al., 1996) and anxiety symptoms (Beinke et al., 2015) among individuals who have encountered a life-threatening health problem. To our knowledge, this is the first study indicating that social constraint may play a role in the appearance of psychological morbidity after an ICU stay.
Multivariate analyses indicated that PTSD symptoms, a stressor-specific distress measure, have different predictors than depressive and anxiety symptoms, both of which are more general measures of distress. Specifically, medical factors and factors related to the experience in the ICU played a role in predicting PTSD symptoms, combined with psychosocial factors, such as gender and SC. A different pattern was observed with anxiety and depressive symptoms. SC and having to deal with other stressors predicted both anxiety and depressive symptoms. In addition, low income was a predictor of anxiety symptoms, highlighting the importance of SES in predicting anxiety when coping with a severe stressor, such as discharge from an ICU (Nikayin et al., 2016). Interestingly, depressive symptoms were negatively predicted by the dose of remifentanil, an analgesic. It may be that perceived helplessness in the ICU, which was a significant predictor of major depressive disorder six months after the ICU stay in another study (Wintermann et al., 2018), rises when attempts at pain management in the ICU are kept at a low level.
LIMITATIONS, FUTURE DIRECTIONS, AND CONCLUSIONS
This study has several limitations. Most importantly, we had a low response rate and a large number of eligible participants who were unable or unwilling to complete the study’s questionnaire, although both are common limitations in studies with ICU patients. Another limitation was the assessment of illness severity with APACHE II, which does not take into account the perceived severity of illness. Furthermore, our findings are based on self-report questionnaires and norms based on data from other cultures. Finally, this study could not clarify whether the negative psychological outcomes reported here are the result of the medical condition which led participants to the ICU or the ICU experience in itself. A strength of the study is the fact that the patients gave their consent while at home, away from the pressure of the hospital, and their participation in the study was not known to the ICU staff at the time of their hospitalization.
Regarding clinical implications, the findings suggest that there is a need for early clinical assessment, especially for patients with strong negative recollections, and with a low SES. As elevated levels of distress during the ICU stay could be indicative of a painful ICU experience and psychological morbidity afterward, clinical assessment should begin while patients are still hospitalized in the ICU, using specialized screening tools (Wade et al., 2014). In addition, psychoeducational interventions should be tailored to individual needs and designed not only for vulnerable patients but also for their caregivers, who may be experiencing high levels of stress and thus be less available to listen and provide support to the patients (Bieleninik et al., 2020; Egerod et al., 2011). Finally, the findings of this study need to be replicated and the impact of SC on psychological morbidity should be researched further in longitudinal studies.
In conclusion, the findings of this study indicate that patients who have been treated in the ICU experience elevated levels of psychological symptoms three months after they are discharged from the hospital. Demographic, psychosocial, and medical factors predicted psychological morbidity. The lack of an available social support system to disclose their hospitalization experiences surfaced as a consistent predictor of psychological morbidity. Being female, coping with additional stressors and low SES also emerged as factors to consider in predicting levels of distress.