BACKGROUND
Adolescents are a particularly sensitive group to suffer mental health alterations, which have become increasingly more evident (Zhou et al., 2020). Approximately 25.0% of adolescents (principally in North America and Europe) suffer from psychological disturbances (Bronsard et al., 2016; Bruffaerts et al., 2018), such as disruptive behaviors, attention deficit and hyperactivity disorder, anxiety and depression among others (Feiss et al., 2019; Pila et al., 2019). In Ecuador, the prevalence of conditions of psychological discomfort is around 15.0%, with conditions of somatization, social dysfunction, anxiety, and alcohol consumption being the most prevalent (Aponte-Zurita & Moreta-Herrera, 2023; Zumba-Tello & Moreta- Herrera, 2022). The causes of these alterations are multifaceted, including modern lifestyle, household income and parenting style, sedentarism and developmental crises (Gesualdo & Pinquart, 2021; Whitney & Peterson, 2019). Moreover, the COVID-19 global crisis has recently exacerbated the predisposition of certain adolescents to suffer mental health problems (Caycho-Rodríguez et al., 2021; Larzabal-Fernandez et al., 2023; Zhou et al., 2020).
Stress is yet another important element to consider, exerting a significant impact as a risk factor (de Figueiredo et al., 2021). Stress is defined as increased arousal resulting from an aversive challenge that is difficult to control, causing fear, anxiety and a physiological reaction (that can lead to coping or fleeing) (Fink, 2010, 2016). The magnitude of the emotional and the physiological response experienced will largely depend on the perception of the event and the individual’s available coping mechanisms (Fink, 2016). In the case of adolescents, about 2/3 show considerable levels of stress, mostly associated with academic matters (Deb et al., 2015). In fact, stress can result from diverse causes, one of the main ones being the educational context, followed by parental and even peer pressure, as well as typical adolescence crises (e.g., authority relationships with parents) (Deb et al., 2015; Saleh et al., 2017)
It is known that chronic exposure to stressful situations in childhood and adolescence has detrimental consequences at the neurological, biochemical (Kim et al., 2013; Romeo, 2017), psychological and behavioral levels (Bourke & Neigh, 2011), in part because they hinder proper maturation. Thus, the association between stress and mental health can be observed both in the general population (Allan et al., 2020; Valentine & Shipherd, 2018) and in young people and adolescents (Anniko et al., 2019; Schwartz et al., 2021). In this regard, evidence suggests that stress plays a role in anxiety, depression and other disorders (Allan et al., 2020; Feiss et al., 2019; Jayanthi et al., 2015), acting as a positive predictor (Saleh et al., 2017; Sánchez-Vélez & Moreta-Herrera, 2022). The underlying mechanism in this relationship is not clear, although emotional mechanisms seem to play a relevant role. For example, exposure to chronic stressful situations (e.g. extreme poverty, intra-familial violence) during childhood and adolescence alters the brain pathways involved in emotional regulation (Kim et al., 2013; Romeo, 2017) and influences the processes of emotional regulation and control (Moreta-Herrera et al., 2022; Young et al., 2019), increasing the number and the intensity of episodes of negative mood with a high presence of negative emotions (Chiang et al., 2017). Moreover, evidence shows that the presence of stress is associated with and predicts negative affect (NA) (Horiuchi et al., 2018), both in adults and adolescents (Anderson et al., 2021; Schwartz et al., 2021; Taylor et al., 2019).
A balanced emotional state is fundamental for integral development, fostering adequate levels of well-being and quality of life (Weinstein, 2018), conceptualized as the presence of positive affect (joy, calm, enthusiasm, others) over NA (anger, frustration, resentment, others) (Sagone & De Caroli, 2014). However, when this pattern is markedly and consistently reversed, mental health alterations arise. This relationship between NA and mental health is evident in adolescents (Arbona et al., 2018; Cho et al., 2017; Fitzsimmons-Craft et al., 2015; Hao & Farah, 2020), triggering and sustaining several mental conditions such as depressive (Anderson et al., 2021), anxiety (Young et al., 2019) or eating (Pila et al., 2019) disorders.
The functioning dynamics of NA could be key to comprehending mental health issues. An elevated presence of NA reflects what Taylor et al. (2019) call a ‘weak brain’, i.e. a brain that is vulnerable to stress (or to situations that might be considered stressful by some, but not by others) and more sensitive to impairment and pathologization. Thus, it could be hypothesized that NA plays a mediating role between stress and mental health alterations, although this has not been demonstrated. In other words, the NA underlies the interaction between these variables, which would help to explain the reason why they remain associated and would allow a deeper understanding of this fact. Therefore, the presence of an indirect effect of stress would even explain the reasons why it is difficult to contain the negative effects on mental health. Nevertheless, it is still commonly accepted that stress has an indirect effect on mental balance and well-being via NA (Arbona et al., 2018). Over the decades, psychological research has shown a preference for the study of direct relationships between variables, while designs that involved third variables in bivariate relationships have been scarcer, limiting the explanatory capacity of the current literature. Furthermore, from the interventional perspective, improving mental health by direct work on restraining stress can sometimes be challenging, so exerting an impact on the indirect pathway through NA could prove useful. Accordingly, the purpose of this study is to deepen our understanding of NA as intervening variables in the stress-mental health dynamic, a phenomenon that, to the best of our knowledge, has not been addressed in adolescents and that represents a notable vulnerability.
OBJECTIVE AND HYPOTHESES
The objectives of this study are: a) to identify the relationships between stress, NA and mental health in Ecuadorian adolescents; and b) to estimate the indirect effect of NA on the stress-mental health dynamic by applying mediation analysis. The following hypotheses are considered: “Stress, NA and mental health are related to each other and conform to a model of good general fit” (H1); and that “NA plays a mediating role in the stress-mental health dynamic” (H2).
PARTICIPANTS AND PROCEDURE
PARTICIPANTS
The sample consisted of 1,154 adolescents, who originally came from 21 cities in Ecuador but at the time of the study lived in the city of Latacunga, Ecuador. 67.7% of the sample were female and the remaining 32.3% were male. The students’ age ranged from 14 to 19 years (M = 15.69 years, SD = 1.06). In addition, the participants identified themselves as either mestizo (91.4%), indigenous (7.2%), white (1.1%) or Afro-Ecuadorian (0.3%). The sample comprised students attending 5 educational centers (82.8% public, 3.4% private and 13.9% religious) in the city of Latacunga, Ecuador. These students were in the first (34.0%), second (34.7%) and third (31.3%) year of high school.
Participants were selected through non-probability sampling according to the following inclusion criteria: a) being students enrolled in the first, second or third year of high school; b) signing an informed consent form to participate in the research; c) voluntarily participating and collaborating in the study.
MEASURES
Negative Affect Subscale (NAS; Watson et al., 1988), as part of the Positive and Negative Affect Scale (PANAS), which has been translated into Spanish (Sandín et al., 1999) and validated in Ecuadorian and Colombian samples (Moreta-Herrera et al., 2021b). This subscale is used to measure the level of NA through a questionnaire of 10 items enquiring about affects such as anger, pain or frustration (e.g., “Do you feel irritated?”; “Do you feel tense?”). Responses are provided through a five-point Likert scale from 1 (not at all or very slightly) to 5 (very much). Its internal reliability in the present study is deemed acceptable with a value of ω = .61, 95% CI [.57; .64].
Perception of Stress Scale (PSS-14; Cohen et al., 1983) and adapted to the Ecuadorian context (Larzabal & Ramos, 2019). This instrument was designed to identify people’s perception of stress through a 14-item questionnaire, where items are grouped into two dimensions: a) perceived stress (PS); and b) stress coping (SC). This instrument assesses each of the items through a five-point Likert scale from 0 (never) to 4 (very often). In the case of the evaluation of the psychometric properties for this work, values of ω = .82 are observed, 95% CI [.81; .84] for PS and ω = .82, 95% CI [.81; .84] for SC, interpreted as acceptable internal consistency.
General Health Questionnaire-28 (GHQ-28; Goldberg & Hillier, 1979), in its Spanish adaptation (Lobo et al., 1986) validated in Ecuador (Moreta-Herrera et al., 2021a). The questionnaire is designed to assess individuals’ perception of general health in primary health care conditions. This 28-item version is configured into four dimensions (somatization, anxiety/insomnia, social dysfunction and severe depression) of seven items each (e.g., “Have you felt perfectly healthy and fit?”; “Have your worries made you lose a lot of sleep?”). Each of the items is answered on a four-point Likert scale from 1 (better than usual) to 4 (much worse than usual). As for reliability in this study, we report values of ω = .86, 95% CI [.85; .87] for somatization; ω = .93, 95% CI [.92; .93] for anxiety/insomnia; ω = .81, 95% CI [.79; .83] for social dysfunction; and ω = .93, 95% CI [.92; .93] for depression. All these values confirm acceptable internal consistency.
PROCEDURE
The research project was disseminated among the participants interested in the study through informative meetings with the prior authorization of the participating institutions. The entire evaluation process was carried out virtually. Participants completed the informed consent form authorized by a legal guardian or representative and an online form collecting sociodemographic data and responses to the psychological tests (NAS, PSS-14 and GHQ-28). Once the evaluations were finalized, the data were filtered and systematized in electronic spreadsheets for the pertinent statistical analyses.
DATA ANALYSIS
The results of the study were obtained in three blocks of statistical analysis. The first one was a descriptive analysis of the variables (see Table 1). The second block of analysis corresponds to the confirmatory factor analysis (CFA) of the measures applied on a matrix of polychoric correlations with maximum likelihood robustness (MLR) estimation given that the data distribution did not present multivariate normality and that the nature of the items was categorical (Li, 2016) (see Table 2). The validity of the scale is interpreted through fit indexes such as the absolute fit indexes: chi-square (χ2), normed chi-square (χ2/df) and standardized root mean square residual (SRMR); as well as relative fit indexes: comparative fit index (CFI) and Tucker-Lewis index (TLI); and a non-centrality-based index: root mean squared error of approximation (RMSEA). Finally, the items’ factor loads (λ) were analyzed to estimate each item’s contribution to the latent construct. Adequate fit was accepted when χ2 was significant (p < .05; although this indicator is sensitive to sample size); χ2/df was lower than 4 (with a tolerance of up to 6); CFI and TLI were greater than .95; SRMR and RMSEA were lower than .06; and the items’ λ were higher than .4 (Brown, 2015; Byrne, 2008; Dominguez-Lara, 2018; Wolf et al., 2013).
Table 1
Descriptive analysis of relevant measures: perceived stress, negative affects and mental health
Table 2
Descriptive analysis of relevant measures: perceived stress, negative affects and mental health
The third block involved the general fit model hypothesized (see Figure 1) and the mediation analysis (see Figure 2) between stress, NA and mental health. Structural equation modeling (SEM) was used for these purposes. In the mediation analysis, the indirect effect (ab) of NA as a mediating variable (M) in the relationship between stress (X) and mental health (Y) was studied. It is considered that there is an indirect effect of M when the ab value is significant (p < .05) and mediation is identified when the direct effect (c’) is lower than the total effect (c) of X on Y. Furthermore, mediation is complete when the c’ value is not significant (p > .05). Otherwise, the pathway is only considered as a partial mediation. The validity of the fit of both the general and the mediation models follows the same criteria as the CFA (Lange et al., 2017).
Figure 1
Final model on perceived stress, negative affects and mental health
χ2 = 823.10***; df = 246; χ2/df = 3.12; CFI = .967; TLI = .963; SRMR = .056; RMSEA = .045 [.042; .049]
Note. Bidirectional lines represent latent relationships, circles represent latent variables and squares represent objective variables. PS – perceived stress; SC – stress coping; Som. – somatization; Ans/In. – anxiety/insomnia; Dis. Soc. – social dysfunction; Dep. – depression; ***p < .001.
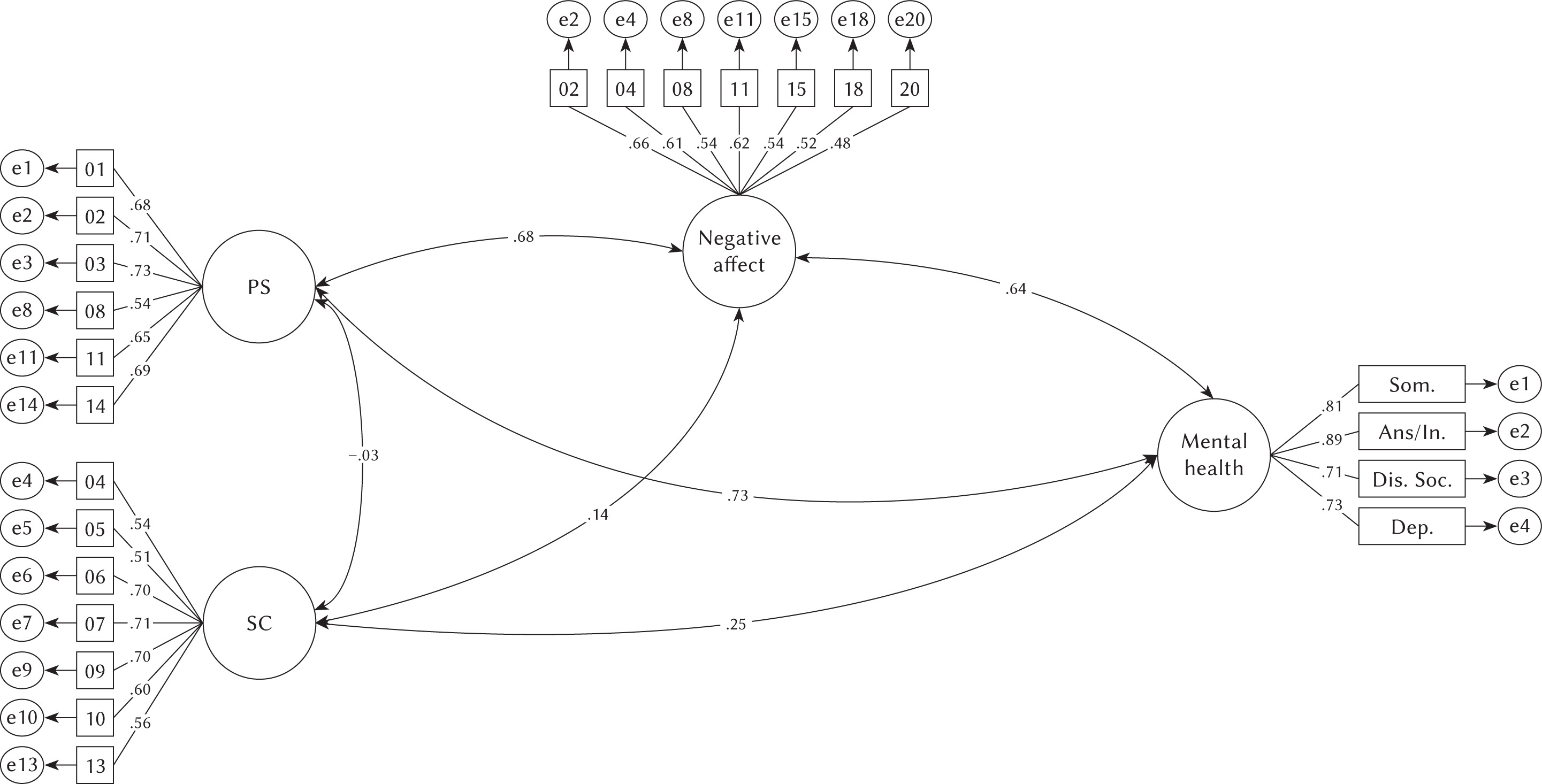
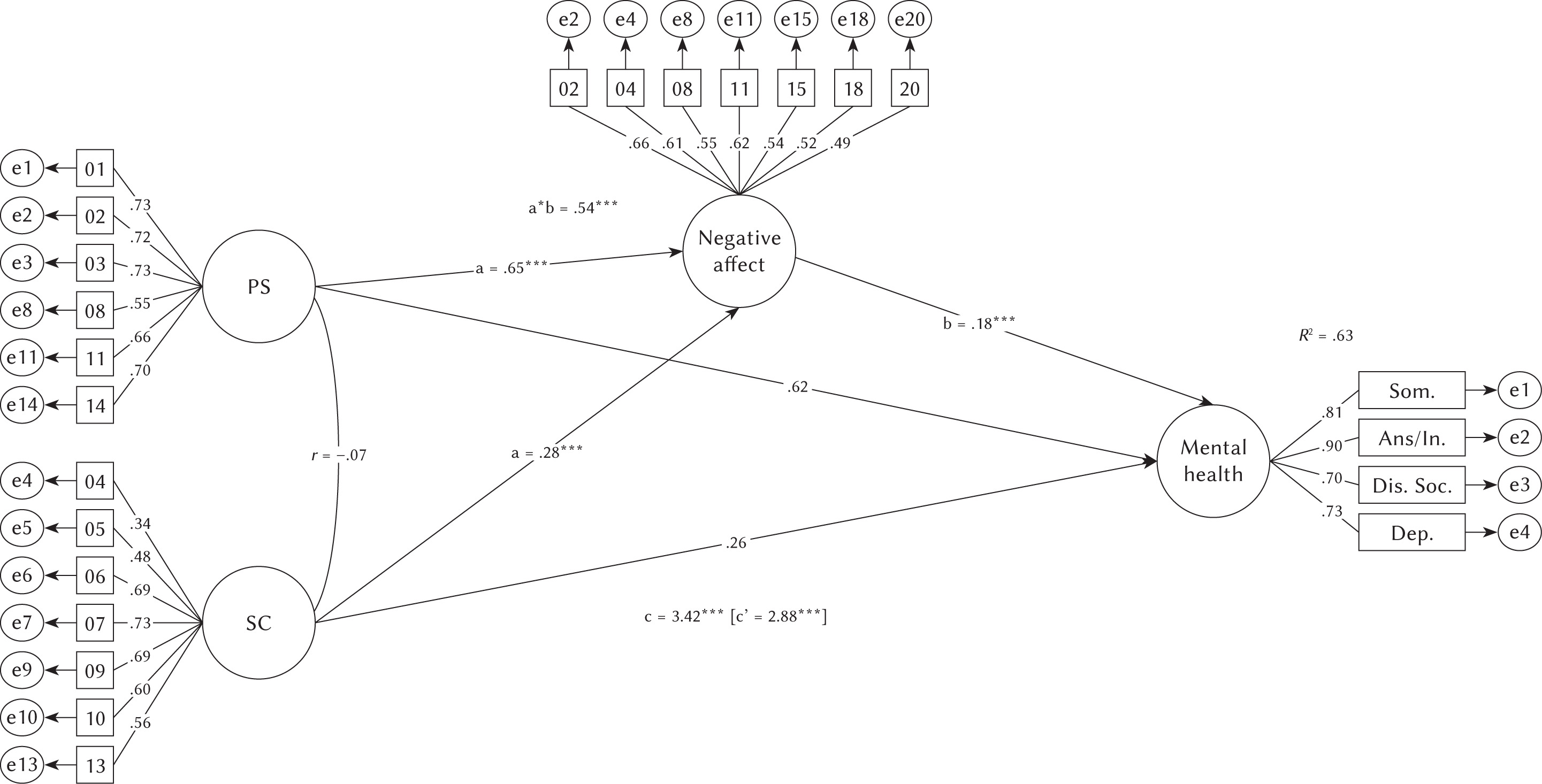
Figure 2
Model of the partial mediation of negative affect in the relationship between stress and mental health
χ2 = 823.10***; df = 246; χ2/df = 3.12; CFI = .967; TLI = .963; SRMR = .056; RMSEA = .045 [.042; .049]
Note. Bidirectional lines represent latent relationships, circles represent latent variables and squares represent objective variables. PS – perceived stress; SC – stress coping; Som. – somatization; Ans/In. – anxiety/insomnia; Dis. Soc. – social dysfunction; Dep. – depression; ***p < .001.
Statistical analyses were performed on R programming language, version 4.0 (R Core Team, 2019) through the following packages: foreign, MNV, lavaan and MBESS.
RESULTS
PRELIMINARY ANALYSIS
Table 1 shows the descriptive analysis of the measures (stress, NA and mental health). In the case of NA, their presence is moderate. Stress criteria show a similar incidence, where the most prevalent dimension is “difficulties in stress coping”. As for mental health, overall, there is a low presence of discomfort and symptoms. However, it should be noted that the most prevalent symptoms (albeit at low levels) are those corresponding to the social dysfunction dimension, followed by somatization. Additionally, multivariate normality is analyzed using the Mardia (1970) test. In this sense, it is observed that in none of the cases is this assumption met, since the results reported for g1 and g2 are significant (p < .05).
CONFIRMATORY FACTOR ANALYSIS
Table 2 analyzes the validity of the internal structure of the measures used in the CFA to build the final model (NA, PSS-14 and GHQ-28). This table shows that, for all tests, the factorial fits were adequate. However, it should be noted that, due to low factor loads, items 5, 9 and 15 from NA were removed, as well as item 12 from PSS-14. In all other cases, saturations were adequate (λ > .50).
GENERAL MODEL FIT
Figure 1 shows the general model fit and the correlations between stress, NA and mental health. The figure shows that NA and perceived stress factors moderately correlate with mental health. Moreover, these variables are more related to symptoms of somatization and anxiety/insomnia than to social dysfunction and depression. Stress coping presents a low correlation with mental health. In addition, perceived stress moderately correlates with NA. These are all positive correlations.
With regards to the final model, the SEM analysis presents adequate fit indexes for the sample under analysis. The items’ factor loads (λ) show that the items that contribute to the latent variables are relevant and significantly contribute to the proposed model.
MEDIATION ANALYSIS
Figure 2 shows the SEM mediation analysis. Given that a*b yields a significant value (p < .001), it is estimated that stress exerts an indirect effect on mental health through NA. In addition, the direct effect (c’) is smaller than the total effect (c), meaning that NA functions as a mediator in the latent interaction between stress and mental health. This is partial mediation, where c’ is significant (p < .001).
On the other hand, the structural regression model shows that the stress and NA exogenous variables explain 62.6% of the variance in mental health as an endogenous variable. Lastly, the final model presents adequate fit indexes and can be considered generalizable to the population of Ecuadorian adolescents.
DISCUSSION
The goal of the present study was to elucidate the relationship between stress, NAs and mental health in a sample of Ecuadorian adolescents. Moreover, the mediating role of NA in the stress-mental health dynamic was also investigated.
In our sample, the presence of NA and stress is moderate. In the case of NA, this is an expected phenomenon among adolescents, due to the emotional difficulties and vital changes associated with this developmental stage (Chiang et al., 2017; Moreta-Herrera et al., 2022; Young et al., 2019). With regards to stress levels, our study shows that this population is frequently exposed to stressful situations. One of the most relevant contributions to stress levels in our sample is connected with coping with situations that are interpreted as stressful, which had been previously described as a typical trait in this stage of life (Fink, 2016). However, if these situations become chronic, there is an increased risk of dysfunction of the brain structures involved in emotional development and mental health (Allan et al., 2020; Valentine & Shipherd, 2018). Finally, in the case of psychological distress and its associated symptoms, their reported intensity is low. That is, the participants’ mental health is not severely affected, although indicators of risk have been detected (where symptoms of social dysfunction and somatization are the most prevalent). This is in accordance with previous works, where adolescents were identified to suffer from mental alterations and probable mental disorders (Bronsard et al., 2016; Bruffaerts et al., 2018; Feiss et al., 2019; Pila et al., 2019). Still, more in-depth and specialized studies on this topic are warranted. In summary, the greater vulnerability of this age group is confirmed and also the fact that they are frequently exposed to situations that put their emotional and psychological stability at risk (Bronsard et al., 2016; Bruffaerts et al., 2018; Zhou et al., 2020).
The final model with SEM (see Figure 1) presents adequate fit indexes’ criteria among adolescents from Ecuador (Brown, 2015; Byrne, 2008; Dominguez-Lara, 2018; Wolf et al., 2013), hence generating an interpretive model of mental health based on stress and NA, using empirical data. In this model, a moderate and positive relationship between stress and NA is confirmed at the latent level. Their covariance is in line with previous studies that obtained a similar outcome, mainly in adolescents and adults (Anderson et al., 2021; Chiang et al., 2017; Schwartz et al., 2021; Taylor et al., 2019). Furthermore, these findings provide relevant information for the studies of Kim et al. (2013) and Romeo (2017), where it was suggested that stress during early life stages alters brain functions associated with affective development.
On the other hand, the model also shows a positive relationship between stress factors and mental health problems in the participants (moderate and low, respectively). That is, stress is related to the disturbance of mental health, as well as to the probable conformation of a specific psychopathology, which is consistent with the findings reported in analogous studies utilizing adult samples (Allan et al., 2020; Valentine & Shipherd, 2018) and adolescent samples (Anniko et al., 2019; Schwartz et al., 2021). Likewise, based on our results, stress presents a stronger relationship with somatization and anxiety/insomnia symptoms than with social dysfunction and depression, which is also in agreement with the studies of Feiss et al. (2019) and Jayanthi et al. (2015). Finally, there is a moderate and positive relationship between NA and mental health. Apparently, the significant presence of NA could trigger the deterioration of mental health in adolescents. These results are in line with preliminary studies that emphasize the relevance of identifying probable prospective negative consequences for mental health (Arbona et al., 2018; Cho et al., 2017; Fitzsimmons-Craft et al., 2015; Hao & Farah, 2020), particularly in the shape of anxiety symptoms and related disorders (Young et al., 2019).
Finally, according to the mediation analysis with SEM (see Figure 2), stress has both a direct and an indirect effect (through NA) on mental health. In this sense, our design captured an important additional element for the understanding of the impact that stress has on mental health. Previously, the study of the indirect effect of stress through NA had already been addressed (Arbona et al., 2018), although not specifically on mental health but on certain specific alterations. Thus, these findings represent a significant advance in the research field analyzing the interaction effect between stress and emotions on mental health and psychopathology in the adolescent population. Furthermore, the proposed model explains 63.0% of the changes in the variance of stress and NA over mental health. Hence it is also confirmed that stress and NA are predictors of mental health status as suggested by Saleh et al. (2017), Sánchez-Vélez and Moreta-Herrera (2022) and Taylor et al. (2019). The relevance of these factors should be taken into consideration in relation to the onset, maintenance and remission of mental problems and alterations.
The results from our study present several important implications. From a theoretical point of view, we propose a novel evidence-based interpretative model for the effect of stress and NA on the mental health of Ecuadorian adolescents. Therefore, this study constitutes a relevant and original contribution, given that this is the first time such an integrative and dynamic theoretical-conceptual model has been proposed. Although it is true that several studies have already analyzed the effect of various predictor variables on mental health, these studies did so independently and utilizing bivariate statistical techniques. Meanwhile, our study proposes a model of latent interaction between variables applying SEM techniques, which has not been attempted before. This approach provides greater precision and facilitates a better understanding of the interaction of these variables. From the practical point of view, our results pose implications for the protocols of mental health assessment which should be followed in case of suspicion of mental health deterioration. Furthermore, our results could lead to the development of preventive and corrective intervention mechanisms for mental health alterations; not only directly, working on stress, but also indirectly addressing the associated emotional response. In this sense, when evidencing that the relationship between stress and SM underlies a negative emotional component among adolescents, public policies in the academic context, as well as in comprehensive health, should be oriented towards the management and control of emotions (both in health promotion, such as prevention, and direct therapeutic assistance), which will positively influence the healthy development of mental health.
LIMITATIONS AND RECOMMENDATIONS FOR FUTURE RESEARCH
This study has a few limitations that should be considered. The first one is related to the specific population approached, which is restricted to adolescents, given that they are deemed as a particularly vulnerable population. In the future, complementary studies on other populations such as older adults, the general population or clinical populations are necessary to elucidate whether the dynamics described here will be sustained or they will change. Similarly, only Ecuadorian adolescents were recruited. For optimal generalization of our results to the wider population of adolescents, cross-cultural validation studies of the mediation model are required, which should include participants from other nations, cultures, and linguistic backgrounds. Despite these limitations, the sample size of this study is a clear strength that suggests that our results should be generalizable at least within its regional context, where research is usually scarce and the population is often understudied. Finally, although the model enables an interpretation in terms of how the independent and mediating variables explain the variance of the outcome variable, due to the specific methodological approach utilized it cannot be stated conclusively that there is a cause-effect relationship between these variables. Future studies are needed to disentangle the nature of these relationships by means of experimental designs or horizontal structural regression studies.