BACKGROUND
In 2020, the Brazilian elderly population represented 14.3% of the population (around 30 million older adults), and it is expected that in 2060 this value will reach 32.2% (around 73 million) (Brazilian Institute of Geography and Statistics [IBGE], 2018). This fast aging of the population poses social and political challenges since the prevalence of chronic diseases, frailty, and disability is higher among long-lived adults (Andrade et al., 2018). Additionally, societal changes (e.g., dual-earner families) have contributed to reducing families’ availability to care for older adults. To address the needs related to older adults’ caregiving, the long-term care facilities for the elderly (LTCFs) have emerged as an important alternative structure. LTCFs are “governmental or non-governmental institutions of a residential nature, intended to provide the collective domicile of persons aged 60 or over, with or without family support, in conditions of freedom, dignity, and citizenship” (The National Agency of Sanitary Surveillance [ANVISA], 2005). The LTCF provides a wide range of services, including rehabilitation, healthcare, personal assistance, and end-of-life care.
Providing care to older adults is an inherently physical and emotionally challenging task. Professionals working in geriatric settings deal with several difficulties including physical and psychological workload as well as arduous working conditions (e.g., Kubicek et al., 2013; Mantzorou & Koukia, 2018; Molina-Praena et al., 2018). For these reasons, health professionals working in assisted living facilities are at greater risk for developing mental health problems. For instance, a review showed that 25-75% of health-care professionals in geriatric settings are likely to experience burnout (Sanchez et al., 2015). Also, a recent study conducted in Brazil showed that almost 20% of the professionals working in long-term care institutions for older adults experienced depression (Borges et al., 2021). Other negative outcomes, such as poor quality of life and stress, have been found within this profession, in comparison to age- and sex-matched populations (see Costello et al., 2019 for a review). However, not every health care professional experiences these types of problems. Indeed, there is great individual variability in the way health professionals experience the demands associated with geriatric care. Individual and job resources are important factors capable of explaining this individual variability.
One important resource that has been explored recently is emotion regulation (ER). ER refers to the process by which individuals “influence which emotions they have, when they have them, and how they experience and express them” (Gross, 1998, p. 271) and has been linked to individuals’ psychological functioning in general (e.g., Brandão et al., 2020; Newman & Nezlek, 2022). However, little is known about how professional caregivers working with older adults regulate their emotions and how those strategies impact workers’ psychological functioning or job outcomes. Some recent studies started to explore these links, with promising results. For example, in a recent daily diary study with 89 geriatric nurses, it was found that cognitive reappraisal was associated with higher subjective well-being and negatively associated with perceived stress; conversely, expressive suppression was negatively associated with well-being and positively associated with perceived stress when the target was positive emotions; when the target was negative emotions no significant associations were found (Katana et al., 2019). In another study conducted with 54 nurses, it was found that ER strategies such as rumination and refocus on planning were associated with lower burnout (specifically in terms of depersonalization) (Bamonti et al., 2022). In other contexts of formal care (e.g., hospitals), ER difficulties were associated with higher emotional exhaustion at work, and higher fatigue and negative affect at home (Blanco-Donoso et al., 2017), while higher ER abilities were associated with more motivation at work and well-being at home even when they faced high emotional demands at work (Blanco-Donoso et al., 2015). Also, in one study with formal caregivers of people with dementia, difficulties in ER were associated with poor physical and mental health (Bassal et al., 2016).
In one study aiming at evaluating the impact of standardized ER training (targeting acceptance, tolerance, and modification of negative emotions) offered to 96 elderly care workers, it was found that improvements in ER skills from pre- to post-treatment were associated with workers’ well-being at the 6-month follow-up (Buruck et al., 2016). For these reasons, we believe that ER can be an important resource explaining individual differences in the mental health of professional caregivers working with older adults.
Another important factor affecting workers’ well-being is work engagement. Work engagement is characterized by three basic components: vigor, dedication, and absorption (Schaufeli et al., 2002). Vigor refers to “high levels of energy and mental resilience while working, the willingness to invest effort in one’s work, and persistence even in the face of difficulties” (Schaufeli et al., 2002, p. 74). Dedication refers to “a sense of significance, enthusiasm, inspiration, pride, and challenge” (Schaufeli et al., 2002, p. 74). Finally, absorption refers to “being fully concentrated and deeply engrossed in one’s work, whereby time passes quickly, and one has difficulties with detaching oneself from work” (Schaufeli et al., 2002, p. 75).
While the specific association between work engagement and mental health of professionals working in geriatric settings has not been explored, the link between work engagement and workers’ mental health, in general, pointed to some important directions. For instance, a 1-year longitudinal study conducted with 8,837 employed individuals found that higher work engagement at baseline was associated with better physical and mental health one year later (Leijten et al., 2015). Other studies with employees have found that work engagement is associated with better mental health, less depression and anxiety (Hakanen & Schaufeli, 2012; Imamura et al., 2016; Innstrand et al., 2012), less psychological distress (Schaufeli et al., 2008), and better sleep quality (Kubota et al., 2010). In one study using a sample of 435 healthcare staff, the links between work engagement and well-being indicators (e.g., psychological well-being and mental resources) were stronger than the links between work engagement and work-related outcomes (Kanste, 2011).
Overall, both ER and work engagement seem to be important factors influencing the mental health of workers in general and professionals working in geriatric settings.
THE PRESENT STUDY
Previous studies have already established associations between ER and mental health of workers (Bamonti et al., 2022; Blanco-Donoso et al., 2015, 2017; Katana et al., 2019) and between work engagement and employees’ mental health (Hakanen & Schaufeli, 2012; Imamura et al., 2016; Innstrand et al., 2012; Kanste, 2011; Leijten et al., 2015). However, there are no studies exploring a more comprehensive and processual approach to these links, especially in the context of geriatric care, which leads to our mediational hypothesis. Because previous research has suggested that ER (especially emotional intelligence) is likely to influence positively work engagement (e.g., Castillo-Gualda et al., 2017; George et al., 2022; Mérida-López & Extremera, 2020), we believe that work engagement may be an important mechanism linking ER to mental health in the context of geriatric care.
Thus, we hypothesize that (H1) expressive suppression (a strategy usually associated with adaptational costs) will be associated with less work engagement (i.e., less vigor, dedication, and absorption), which in turn will be associated with poor mental health (i.e., more depression, more anxiety, and more stress); on the other hand, we expect that (H2) cognitive reappraisal (a strategy usually associated with better outcomes) will be associated with more work engagement (i.e., more vigor, dedication, and absorption), which in turn will be associated with better mental health.
PARTICIPANTS AND PROCEDURE
PARTICIPANTS
A total of 104 professionals working in 13 long-term care facilities for the elderly in Brazil were included in this study. Most were female (n = 85, 81.7%), with a mean age of 37.93 (SD = 10.57). Most were single (n = 42, 40.4%) or married (n = 36, 34.6%) and lived in an urban area (n = 98, 94.2%). In terms of education, 39.4% (n = 41) had a higher education degree and 55.8% (n = 58) had a secondary education. In terms of profession, most were caregivers (n = 36, 34.6%), followed by nurses (n = 15, 14.4%) or nurse technicians (n = 32, 30.8%). Most of the participants had worked in the institution for more than 3 years (n = 43, 43%; M = 37.00 months, SD = 44.86; min = 1 month, max = 264 months) and worked shifts (n = 77, 74%).
MEASURES
Sociodemographic (age, education, marital status, living area) and work-related information (profession, time working at the institution, shift work) were collected through participants’ self-report.
The Depression, Anxiety and Stress Scale. Depression, anxiety, and stress were measured using the Depression, Anxiety and Stress Scale – 21 Items (DASS-21; Lovibond & Lovibond, 1995; Brazilian version: Vignola & Tucci, 2014). The DASS-21 is a self-report scale composed of 21 items divided into three subscales. Each subscale consists of seven items that measure the emotional states of depression (item example: “I couldn’t seem to experience any positive feeling at all”), anxiety (item example: “I felt scared without any good reason”), and stress (item example: “I felt that I was using a lot of nervous energy”). Items are scored on a Likert-type scale ranging from 0 (strongly disagree) to 3 (totally agree). In the present study, Cronbach’s α was .79 for depression, .83 for anxiety, and .83 for stress.
The Emotion Regulation Questionnaire. Emotion regulation was measured using the Emotion Regulation Questionnaire (ERQ; Gross & John, 2003; Brazilian version: Boian et al., 2009). The ERQ is a self-report scale composed of 10 items that measure expressive suppression (i.e., efforts to inhibit ongoing emotion-expressive behavior; 4 items; item example: “I keep my emotions to myself”) and cognitive reappraisal (i.e., efforts to change a potentially emotion-eliciting situation with the aim of changing its emotional impact; 6 items; item example: “When I’m faced with a stressful situation, I make myself think about it in a way that helps me stay calm”). Items are scored on a Likert-type scale ranging from 1 (strongly disagree) to 7 (strongly agree). In the present study, Cronbach’s α was .62 for expressive suppression and .71 for cognitive reappraisal.
The Utrecht Work Engagement Scale. Work engagement was measured with the Utrecht Work Engagement Scale (UWES-17; Schaufeli & Bakker, 2004; Brazilian version: Vazquez et al., 2015). The UWES is a self-report scale composed of 17 items that measure three subscales: vigor (6 items; item example: “At my job, I feel strong and vigorous”), dedication (5 items; item example: “I am enthusiastic about my job”), and absorption (6 items; item example: “Time flies when I’m working”). Items are scored on a Likert-type scale ranging from 1 (never) to 7 (always). In the present study, Cronbach’s α was .84 for vigor, .79 for dedication, and .66 for absorption.
PROCEDURE
This study was approved by the Ethics Committee at the Psychological Research Center of the Autonomous University of Lisbon (reference: 08-2020). A total of 50 institutions were contacted; however, only 13 approved the study. Participants were invited by institutions’ administrators to participate in the study both by email and, in some cases, in person. Data were collected using Google Forms. The main goals of the study were presented on the landing page. Written informed consent by participants was required to proceed with the survey. Participation was voluntary – no incentives or compensation were offered, and confidentiality was ensured.
DATA ANALYSIS
Data were analyzed using IBM SPSS (version 26). Descriptive and bivariate correlations among study variables were examined using descriptive statistics (means and standard deviations) and Pearson correlations.
The multiple mediation models were examined using the PROCESS macro (version 3.4) from Hayes (2015). PROCESS model 4 was used to test various models. The independent variables were cognitive reappraisal and expressive suppression (ERQ), the mediation variables were vigor, dedication, and absorption (UWES-17), and the dependent variables were depression, anxiety, and stress (DASS-21). Total, direct, and indirect effects were examined. Indirect effects were tested using bootstrapping with 5000 bootstrap samples and were considered significant if the 95% bias-corrected confidence intervals did not include 0.
RESULTS
DESCRIPTIVE STATISTICS
Descriptive statistics are presented in Table 1.
Table 1
Means, standard deviations, and correlations among emotion regulation, work engagement, and mental health
CORRELATIONS
Expressive suppression was positively associated with cognitive reappraisal and vigor, and negatively associated with depression, anxiety, and stress. Cognitive reappraisal was positively associated with vigor and dedication, and negatively associated with depression, anxiety, and stress.
Vigor was positively associated with expressive suppression and cognitive reappraisal, dedication, and absorption, and negatively associated with depression, anxiety, and stress. Dedication was positively associated with cognitive reappraisal and with absorption, and negatively associated only with anxiety. Depression was positively associated with anxiety and stress. Anxiety and stress were also positively associated.
Length of service in the institution was not correlated with any study variables; thus it was not included in the mediational analyses (see Table 1).
MULTIPLE MEDIATION MODELS
Expressive suppression models. Expressive suppression was significantly associated with vigor (esti-mate = .14, p = .023) but not with dedication (esti-mate = .07, p = .204) or absorption (estimate = .08, p = .188). Also, expressive suppression was significantly associated with depression (estimate = –.70, p = .005), with anxiety (estimate = –.61, p = .013), and with stress (estimate = –.83, p = .004). When the mediators were considered, these associations remained significant (depression estimate = –.51, p = .033; stress estimate = –.56, p = .041), except for anxiety (estimate = –.33, p = .138). Vigor was significantly associated with depression (estimate = –1.76, p = .008), anxiety (estimate = –2.68, p < .001), and stress (estimate = –2.50, p < .001); dedication was associated with depression (estimate = 1.45, p = .018); the remaining associations were not significant (see Figure 1).
Figure 1
Multiple mediation models with expressive suppression, work engagement, and mental health
Note. *p < .05, ***p < .001.
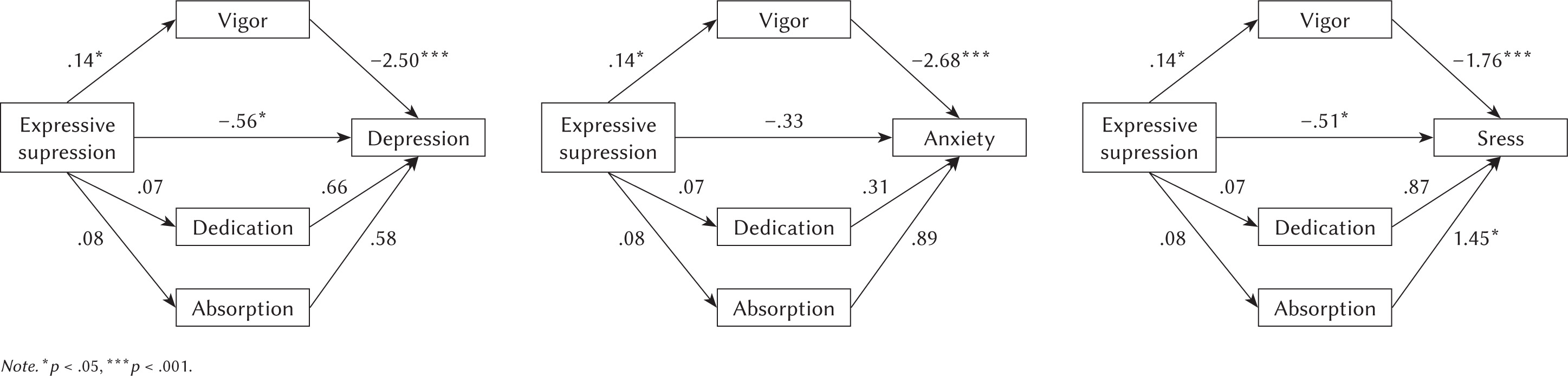
Indirect effects (presented in Table 2) showed that vigor (but not dedication or absorption) partially mediated the association between expressive suppression and stress, and totally mediated the association between expressive suppression and anxiety.
Table 2
Indirect effects of emotion regulation (expressive suppression) on mental health (depression, anxiety, and stress) via engagement (vigor, dedication, and absorption)
The first model explained 22% of the variance of depression (F(4, 99) = 6.86, p < .001); the second model explained 28% of the variance of anxiety (F(4, 99) = 9.68, p < .001); the third model explained 20% of the variance of stress (F(4, 99) = 6.37, p < .001).
Cognitive reappraisal models. Cognitive reappraisal was significantly associated with vigor (esti-mate = .29, p < .001) and dedication (estimate = .22, p < .001) but not with absorption (estimate = .13, p = .061). Also, cognitive reappraisal was significantly associated with depression (estimate = –1.27, p < .001), with anxiety (estimate = –1.05, p < .001), and with stress (estimate = –1.20, p < .001). When the mediators were considered, these associations remained significant (depression estimate = –.86, p = .003; estimate = –.54, p = .051; stress estimate = –.83, p = .017). Vigor was significantly associated with depression (estimate = –1.52, p = .020), anxiety (estimate = –2.54, p < .001), and stress (estimate = –2.31, p = .003); the remaining associations were not significant (see Figure 2).
Figure 2
Multiple mediation models with cognitive reappraisal, work engagement, and mental health
Note. *p < .05, **p < .01, ***p < .001.
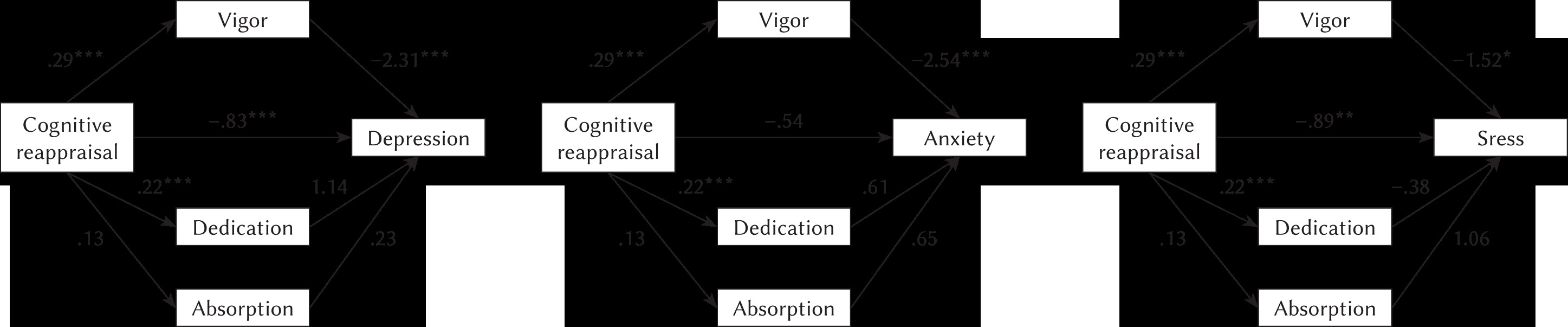
Indirect effects (presented in Table 3) showed that vigor (but not dedication or absorption) partially mediated the association between cognitive reappraisal and stress and between cognitive reappraisal and anxiety. The first model explained 25% of the variance of depression (F(4, 99) = 8.27, p < .001); the second model explained 54% of the variance of anxiety (F(4, 99) = 10.25, p < .001); the third model explained 22% of the variance of stress (F(4, 99) = 6.86, p < .001).
Table 3
Indirect effects of emotion regulation (cognitive reappraisal) on mental health (depression, anxiety, and stress) via engagement (vigor, dedication, and absorption)
DISCUSSION
The present study examined the associations between ER, work engagement, and mental health among a sample of health professionals working in long-term care facilities in Brazil. While previous studies have identified associations between ER (especially emotional intelligence) and work engagement or mental health and between work engagement and mental health, to the best of our knowledge, no studies have explored a mediational and processual model, specifically in the context of geriatric care in long-term care facilities. First, in line with previous studies in other professional contexts, our results showed a significant association between ER and work engagement (Castillo-Gualda et al., 2017; George et al., 2022; Mérida-López & Extreme-ra, 2020). Specifically, expressive suppression was positively linked to vigor and cognitive reappraisal was positively linked to vigor and dedication. The results regarding expressive suppression are quite interesting since it was associated with more vigor, contrary to our predictions. Expressive suppression is usually a costly ER strategy associated with negative intrapersonal and interpersonal outcomes (e.g., Chervonsky & Hunt, 2017; Hu et al., 2014). However, in our study, it was associated with more vigor and less depression, anxiety, and stress (H1 was not confirmed), suggesting that it can have an adaptational role for professionals working in a geriatric context. It is possible to hypothesize that in contexts marked by heavy workloads and challenges in the work environment, such as those faced by workers of long-term care facilities, the use of expressive suppression may be beneficial. Indeed, this pattern has been found in previous studies with rescue workers who believed that complaining and ‘venting’ would be more prejudicial for their work than suppressing their emotions because it would increase their resentment and their negative affect regarding their job (Gan et al., 2014; Moore et al., 2008). It is important to note, however, that these studies were conducted in a Western culture in which suppression is valorized, and is usually associated with more positive outcomes (Hu et al., 2014). Yet, some studies have suggested that the suppression of emotions may be important to maintaining relationships and employment (Gross, 2002; Gross & John, 2003).
A similar pattern was found in a sample of medical students; when they faced a negative incident with patients associated with negative emotions, they tended to use different strategies, one of them expressive suppression which allowed them to be efficient in the task they had to perform or to make better decisions (Doulougeri et al., 2016). Thus, it is possible that concealing one’s emotions contributes to higher levels of vigor in terms of resilience and persistence to deal with work demands.
Additionally, our results showed that expressive suppression and cognitive reappraisal were positively associated, suggesting that individuals use both types of strategies. Thus, we can hypothesize that when expressive suppression is used in a flexible way, along with other strategies (such as cognitive reappraisal), it can lead to more positive outcomes. Previous studies have suggested that is the habitual and inflexible use of expressive suppression that is associated with negative outcomes (e.g., Bonanno et al., 2004).
With regards to cognitive reappraisal, our results are in accordance with previous studies (allowing the confirmation of H2) suggesting that this type of strategy is usually adaptive. A positive association between cognitive reappraisal and work engagement has been found in previous studies within other professional contexts (e.g., teaching; Burić & Macuka, 2018; Greenier et al., 2021). This result seems to suggest that professionals who can cognitively reframe situations and change their meaning in a more positive way are more likely to be involved in their profession (in terms of vigor and dedication). Additionally, the positive link between cognitive reappraisal and mental health has also been found in previous studies, including with health care professionals (Katana et al., 2019). In Katana’s study, the content analysis demonstrated that cognitive reappraisal contributes to increasing the experience of more positive emotions and reduce the experiencing of negative emotions, which can promote well-being and decreases perceived stress.
Finally, we found that emotion regulation (in terms of both expressive suppression and cognitive reappraisal) influenced mental health (specifically anxiety and depression) via vigor. These results seem to suggest that workers who are more capable of regulating their emotions (using both expressive suppression and cognitive reappraisal in a flexible way according to work demands) are more likely to be resilient, invest in their profession, and be persistent in the face of difficulties. This, in turn, contributes to protecting them from experiencing anxiety and stress. Indeed, the model of emotion regulation flexibility proposed by Aldao et al. (2015) suggested that the adaptiveness of emotion regulation strategies will depend on the context in which they are used as well as on the motives/goals underlying the choice of emotion regulation strategies.
LIMITATIONS AND FUTURE RESEARCH
To more accurately understand the results presented, several limitations should be noted. First, this is a cross-sectional study, and, for this reason, we cannot infer causality. Longitudinal studies should be conducted to establish a temporal sequence among study variables and examine how they interact over time. Second, this study relied only on self-report data. A qualitative approach should be further employed to better understand relationships among study variables. Indeed, as reported previously, some studies with qualitative data have provided some clues on why professionals benefit from both expressive suppression and cognitive reappraisal. Future qualitative studies should be conducted to better understand the motive underlying the use of these strategies to understand why they are linked to work engagement and, consequently, to mental health.
Also, our sample was composed mainly of women and caregivers, nurses, and nurse technicians. Future studies should include a more equal diverse sample and, possibly, examine whether the sex or profession moderates the associations between emotion regulation, work engagement, and mental health in workers of long-term care facilities.
Finally, no description of the institutions was obtained (e.g., ratio of users/professional, type of users in terms of degree of dependency). Thus, it is possible that the institutions that agreed to participate in the study were those with a lower workload or better conditions, limiting the results.