BACKGROUND
Parental responsiveness has been studied for decades, as it plays a crucial role in providing the physical and psychological needs of an infant (Ainsworth et al., 1974). Since parental responsiveness is a complex concept, it might manifest differently depending on the context, as do other parenting behaviors (Shai, 2019). It can be studied in interactions, in situational contexts, through simulations, or with self-report scales. However, there is a lack of studies that combine objectively judged behaviors in situational contexts with self-report scales involving the family triad (i.e., the parents and the child). It is important to distinguish a parent’s self-perception of their own responsiveness from the real responsive behaviors they display towards their child. In the present study, we aimed to test whether observational and self-report assessments of maternal and paternal responsiveness agree with each other, and also whether individual differences in empathy and attachment in mothers and fathers and their satisfaction with their relationship are predictors of parental responsiveness toward infants.
Children explore the world in the presence and with the support of a parent (Bakermans-Kranenburg & van IJzendoorn, 2015). Parent-child positive emotional synchrony supports early childhood emotional development. Research has shown that parents who are responsive to their children tend to have children who are more socially competent, have better relationships with their peers, and have better mental health outcomes (Kaźmierczak et al., 2007).
Responsive parents are always ready to perceive their child’s needs, are attuned to respond to them adequately, and adapt to the child’s activity level (Belsky & Barends, 2002). The child’s cues and states depend on environmental variables (e.g., the closeness of a parent), so these interactions always occur in a situational context. The responsive parent creates an environment for development based on the child’s needs. The parent pays attention to the child and, crucially, the parent is present in the moment with the child. The responsive parent provides a warm and nurturing environment, encourages and supports the child’s autonomy and independence, and pays attention to the child’s interests. Parents should also provide many opportunities for learning and exploration. However, they should set clear and consistent boundaries and rules. A responsive parent gives their child sufficient indication from the beginning that the child’s actions can affect their surroundings and that the parent can provide help if the child experiences discomfort (van IJzendoorn & Bakermans-Kranenburg, 2012). The opposite behaviors, such as trying to play with the child when he/she is tired or hungry, or feeding when the child wants social interaction, interfere with the child’s needs and may lead to frustration (Belsky, 2014). Parents who are less responsive and have less positive experiences during family activity present lower conflict resolution, caused by lower engagement and perseveration of negative emotions (Low et al., 2019).
Attachment is another important factor for parental responsiveness. Attachment is a strong and enduring emotional bond between a child and their primary caregiver (Kucharska, 2021), and it influences the child’s later development. An insecure pattern of attachment in parents increases the risk of being less responsive and supportive to their children. Mothers who are avoidant and anxious in their close relationships display higher levels of avoidance and anxiety also to their children and are less responsive to them (van IJzendoorn & Bakermans-Kranenburg, 2012).
Parental responsiveness is conditioned by a person’s individual dispositions, such as their empathy (Kaźmierczak et al., 2015). Indeed, being responsive necessitates empathizing with one’s child, taking his/her perspective, and responding with compassion and concern. Several studies have shown that parents who are able to empathize with their child’s feelings of sadness may respond by offering comfort and support, rather than dismissing or invalidating their child’s emotions. As previous studies have revealed, a higher level of empathy is linked with greater sensitivity to cues coming from the child (Boorman et al., 2019). In this paper, we follow the dispositional empathy definition of Davis (2004) and refer to other-oriented empathic concern (compassion and care for others; Davis, 2004) and perspective-taking (taking others’ points of view in social situations; Davis, 2004), which may help parents to respond to a child’s cues adequately (Stern et al., 2015). Empathic concern facilitates parental responsive reactions such as monitoring and perceiving the child’s cues (Eisenberg & Eggum, 2009). Perspective-taking has been found to be associated with observed maternal responsiveness in a naturalistic context as well as with more self-reported child-oriented empathy and less self-oriented parental emotional reactions to an infant crying (Kaźmierczak & Pawlicka, 2019). On the other hand, self-oriented personal distress, as a component of empathy, refers to the discomfort or anxiety that an individual feels when they are confronted with another person’s negative emotions (Davis, 2004), including their child’s crying and frustration. Furthermore, parental other-oriented empathy predicts elevated levels of responsiveness during interaction with a crying child simulator (Kaźmierczak et al., 2022).
Parents who are more responsive toward their children are also more responsive to their partners/spouses. This suggests that individual differences play a key role in communication and responsiveness to others’ needs (Estlein & Theiss, 2020). As previous studies have shown, empathy is also linked to a higher quality of intimate relationships, especially regarding communication and support (Verhofstadt et al., 2016). The emotions experienced by partners after the birth of a child are associated with satisfaction in the relationship (Kaźmierczak, 2015). Moreover, the quality of parental relationships helps men adapt to the role of being a father (Kaźmierczak, 2015). The participation of fathers in the lives of their children has increased in the last two decades, but in some families their role remains modest (Buisman et al., 2022). Several studies on fathers’ responsiveness have shown that they are less responsive than mothers (e.g., Schoppe-Sullivan et al., 2006), both in terms of their individual dispositions and the quantity of their interactions with the child. However, one intervention study demonstrated that assisted interactions between a father and his baby is a promising strategy for improving sensitive fathering in the early postnatal phase (Buisman et al., 2022). Nevertheless, the topic of parental responsiveness should be further explored.
It should be underlined that the period after the child’s birth (including especially the first year of the child’s life) can be very demanding and emotionally draining, and requires a lot of personal resources. The support that parents receive from their relationships is crucial for their adaptation and readiness to be responsive (Ruan et al., 2020). With the help of a partner, it is also easier for parents to take care of themselves in order to be able to effectively care for their children. When parents are able to manage their own emotions and needs, they are better able to provide a supportive and nurturing environment for their children.
Couples’ relationship problems can bias perceptions of a partner’s responsiveness toward the child. Misunderstanding and lack of empathy are risk factors for underappreciating a partner’s abilities. This can result in decreased ability to provide a connected, stable, and secure family environment (Cross et al., 2021).
In this study, we compared observational and self-assessed parental responsiveness towards their child in first-time-parent couples, expecting similar results for both measures. We first tested whether the different measures of parental responsiveness (self-report and observational) were congruent. We then examined the following hypotheses:
H1. Mothers are more responsive than fathers for both observational and self-assessed measures.
H2. Higher empathic concern and perspective taking in parents are positively correlated with higher responsiveness to their child for both observational and self-assessed measures.
H3. Higher attachment avoidance and anxiety in a parent are linked with lower parental responsiveness for both observational and self-assessed measures.
H4. Higher satisfaction in partners is connected with higher parental responsiveness for both observational and self-assessed measures.
We also examined the actor and partner effects.
PARTICIPANTS AND PROCEDURE
PROCEDURE
A standardized procedure was designed to control the influence of external factors. The study was conducted in a laboratory arranged like a child’s room with a one-way mirror at the University of Gdansk. In the room were two cameras to provide a whole picture of the situation. With this setup, it was possible to observe the interaction between the parent and child. The cameras also recorded the session to allow assessment of every aspect of the interaction between the parent and infant. The free play lasted 10 minutes. Parents were asked to “play and spend this time with their children as usual”. The laboratory was always arranged in the same way (i.e., the same arrangement of toys and furniture) and each parent received the same set of toys (e.g., rattles, books, animal figurines). While one parent was interacting with the child, the other completed a set of questionnaires in a room next to the examination room. Then, they switched places.
MEASURES
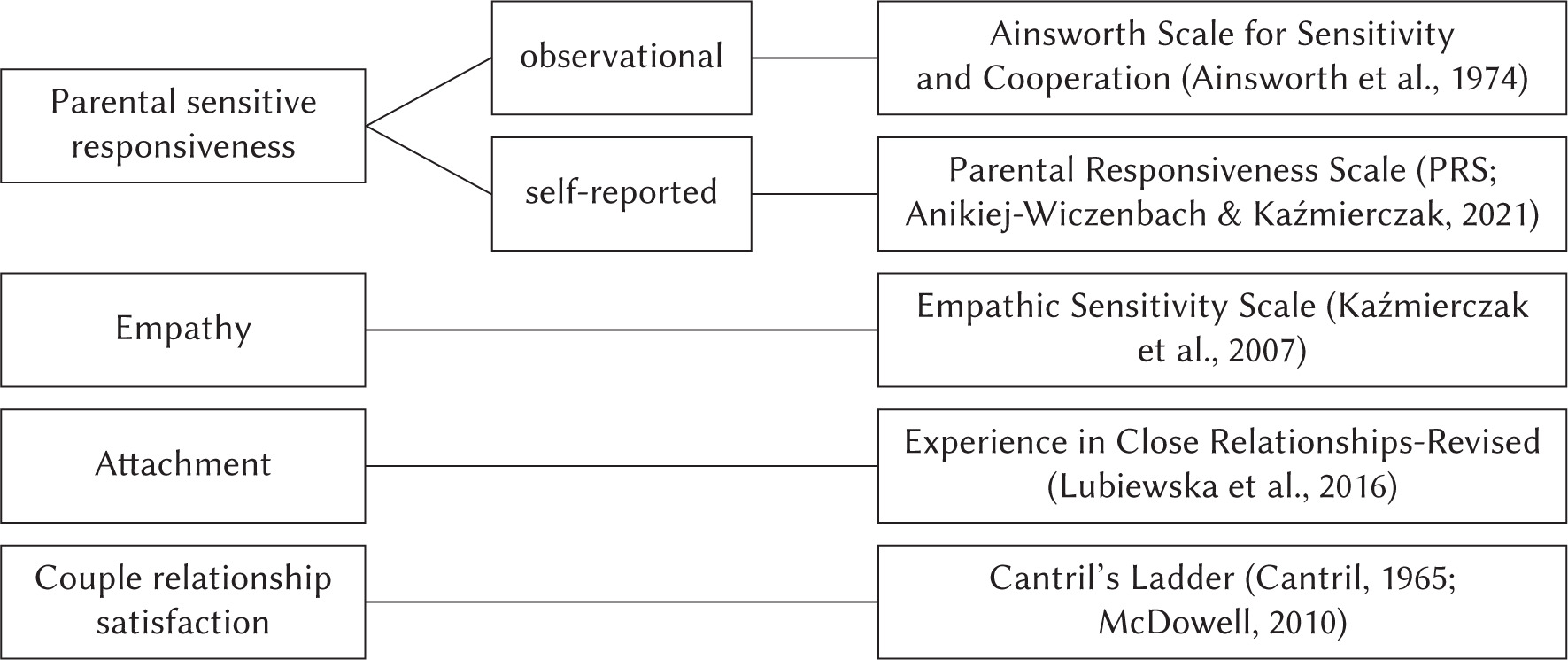
Parental sensitive responsiveness. This variable was measured both observationally and through self-report. After conducting the free-play procedure, the researcher assessed parental sensitivity based on the behaviors displayed towards the child using the recorded footage. Assessment of the scores was done following the Ainsworth Scale for Sensitivity and Cooperation (Ainsworth et al., 1974). The scale ranges from 1 to 9 points (for sensitivity, 1 corresponds to highly insensitive and 9 to highly sensitive; for cooperation, 1 corresponds to highly interfering and 9 to highly cooperative). Every behavior towards the infant performed by parents was described (the entire recording was analyzed) and, in the next step, interpreted as sensitive, insensitive, cooperative, intrusive, or neutral. Also, missing cues or opportunities to be responsive was noted. Then, regarding the descriptions, parents received points for their sensitivity and cooperation during this observation. The Sensitivity vs. Insensitivity Subscale measures a parent’s ability to distinguish and interpret signals accurately, to identify the infant’s implicit attitude, and to respond to them appropriately and promptly. This scale measures the following components: 1) awareness of signals; 2) accurate interpretation of cues; 3) appropriate responses; and 4) promptness of reactions. An example of a behavior that could be coded as sensitive would be “The parent observes the gaze of the child and responds with an encouraging smile when their gazes meet.” An unresponsive behavior would be “The parent does not notice the child’s gaze because they were on their mobile phone.” The Cooperation vs. Interference with Baby’s Ongoing Behavior Subscale also has a nine-point scale from 1 (highly interfering) to 9 (highly cooperative). This scale measures the degree to which parental interventions interrupt or cut short the baby’s activities in contrast to responding adequately and at a time appropriate to the baby’s state, mood, and interest. The interference was assessed in terms of two aspects: 1) physical interference with the baby’s current activity and 2) frequency of interruptions. A cooperative behavior would be “The child throws the ball again and the parent continues this play with him.” An interfering behavior would be “The parent interrupts the child’s play with a toy when he is still interested in it, introducing a book.” To avoid comparing responsiveness between parents, people from the same family were coded by two different researchers. Additionally, there was a 30% overlap to assess the coders’ reliability.
Parents also assessed whether they perform responsive reactions to the infant’s cues on the seven-point (1 – I disagree; 7 – I strongly agree) Parental Responsiveness Scale (PRS; Anikiej-Wiczenbach & Kaźmierczak, 2021). Sample statements include: “I immediately react to the cry of my child,” “I reciprocate the smile of my child,” “I name the objects indicated by the child,” and “I make contact with my child when I see that he/she wants it.” In this study, the tool displayed good reliability and internal and external accuracy. The value of α was .87 for women and .82 for men.
Empathy. The Empathic Sensitivity Scale (Kaźmierczak et al., 2007) was used to measure empathy in both parents. This questionnaire consists of 28 items; participants responded to these statements using a five-point Likert response scale. Results were obtained for three subscales (components of dispositional empathy): 1) Empathic Concern – other-oriented emotional empathy (showing sympathy and concern to people in difficult situations; e.g., “I often have tender, concerned feelings for people less fortunate than me”); 2) Perspective-taking – other-oriented cognitive empathy (taking other people’s points of view; e.g., “Sometimes I try to understand my friends better by imagining the situation from their point of view”); and 3) Personal Distress – self-oriented emotional empathy (the experience of negative emotions in response to others’ discomfort or suffering; e.g., “When I see someone who badly needs help in an emergency, I go to pieces”). All subscales are characterized by satisfactory reliability: .83 for empathic concern, .76 for personal distress, and .81 for perspective taking in women; and .73 for empathic concern, .75 for personal distress, and .71 for perspective taking in men.
Attachment. Experience in Close Relationships-Revised (ECR-R – short version; Lubiewska et al., 2016). The scale is composed of 16 items. Participants are assessed on a seven-point Likert scale (1 – extremely untrue; 7 – extremely true) regarding attachment patterns in close relationships, based on avoidance and anxiety indicators. An example of a statement from the avoidance subscale is “I start to feel uneasy when someone important to me wants to be very close.” An example from the anxiety subscale is “I’m afraid I will lose the love of someone dear to me.” In this study, the values of α were .86 for attachment anxiety and .84 for attachment avoidance for women, and .86 for anxiety and .85 for avoidance for men.
Couple relationship satisfaction. Data about satisfaction within relationships were gathered using the modified version of Cantril’s Ladder (Cantril, 1965; McDowell, 2010). This consists of a visual representation of a ladder with ten rungs, each representing a different level of satisfaction. The top rung represents the highest level of satisfaction, while the bottom rung represents the lowest level of satisfaction. In this study, α was .90 for women and .88 for men.
All parents provided socio-demographic data, impressions related to the perinatal period and delivery, and data about the child’s health. The measures used in this study are presented in Figure 1.
PARTICIPANTS
A total of 110 triads (mother, father, and their first and only child; N = 330) participated; the children were aged from 6 to 10 months (M = 7.49, SD = 1.15), including 61 (55.45%) parents of girls. The children had been born between 37 and 42 weeks (M = 39.95, SD = 1.30). Most of them (n = 78; 70.3%) were born through vaginal delivery, and the rest of them were born by caesarean section. The exclusion criteria were diseases and developmental abnormalities, and one family was excluded because they did not meet this criterion. The mothers were aged 20 to 41 years (M = 29.91, SD = 3.62) and the fathers were aged 25 to 50 years (M = 31.20, SD = 3.77). They had been in close relationships for between 1 year and 23 years (M = 7.47, SD = 3.99). The majority of parents had higher education (for mothers n = 91 and for fathers n = 77), some of them had secondary education (for mothers n = 11 and for fathers n = 11) or vocational education (for mothers n = 7 and for fathers n = 20), and a few of them had primary education (for mothers n = 1 and for fathers n = 2). The majority of women were working (n = 95; 85.6%) and all fathers were working. A total of 91 (82%) parents were married and the rest of them were cohabitating; 81% of families were living in a city and the rest of them were living in the countryside; 82% (n = 91) of families stated that their pregnancy was planned, 16.2% (n = 18) stated that their pregnancy was unplanned but expected, and 1 stated that they had not been expecting the child. For the majority of couples, it was the first pregnancy (n = 94; 84.7%), for 11 couples (9.9%) it was the second pregnancy, and for 5 there had been more than two unsuccessful pregnancies; 21 (18.9%) couples reported having had difficulty conceiving and 11 (9.9%) of them received fertility treatment. The characteristics of the study group are summarized in Table 1.
Table 1
Characteristics of study group
Parents were recruited in antenatal schools in the Pomeranian area and through advertisements on social media. As compensation, they received a description of the functioning of the child. The diagnosis of the psychosocial functioning of the child was conducted after the study with a standardized research tool (Observation Scale from the Children’s Developmental Scale; Matczak et al., 2007).
DATA ANALYSIS
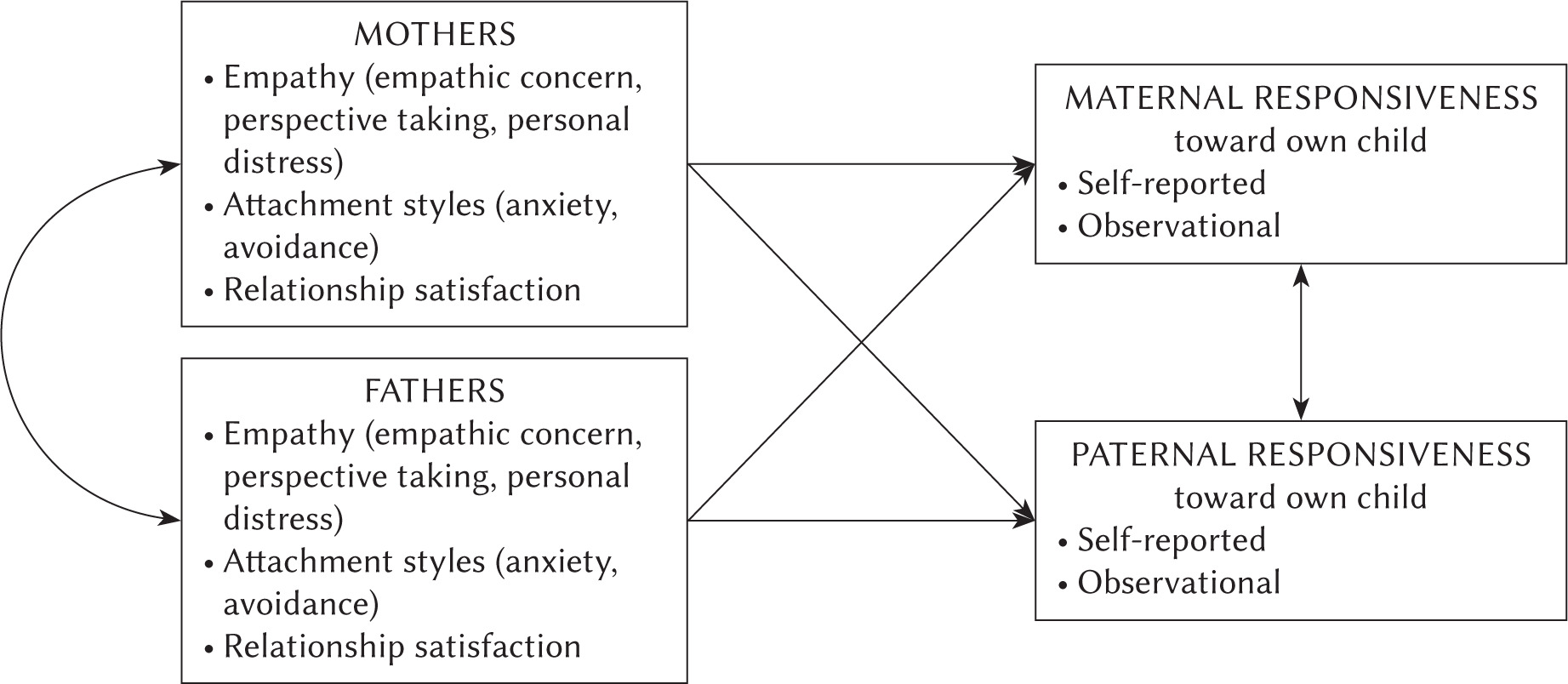
SPSS 27.0 was used to calculate the means, standard deviations, Pearson correlation coefficients, and dependent samples t-tests. Nine different actor-partner interdependence models (APIMs; Cook & Kenny, 2005) were tested: three where empathy dimensions were the independent variables and sensitivity, cooperation, and parental responsiveness (measured with PRS) were the dependent variables; three where attachment dimensions were the independent variables and sensitivity, cooperation, and parental responsiveness (measured with PRS) were the dependent variables; and three where relationship satisfaction was the independent variable and sensitivity, cooperation, and parental responsiveness (measured with PRS) were the dependent variables. The theoretical model of this study is presented in Figure 2. The APIM is a statistical method that tests interdependence in a relationship. The two major effects within APIMs are actor effects and partner effects. The actor effect is intrapersonal and is the effect of an individual’s independent variable on their dependent variable. The partner effect is interpersonal and is the effect of a partner’s independent variable on an individual’s dependent variable. The APIMs were tested using the lavaan 0.6-12 package (Rosseel, 2012) for R 4.2.0 (R Core Team, 2022) with the robust maximum likelihood (MLR) estimator. All tests were two-tailed, and the significance level was set to α = .05. The figure showing the APIM for this study is in the Supplementary materials.
RESULTS
Firstly, the congruency of the measurements of parental responsiveness were analyzed. For the observational scale, there was a strong correlation between sensitivity and cooperation in both women and men (Table 2). There were also positive associations between observed and self-reported sensitivity in dyads. However, at the individual level, no significant correlations were found between observed and self-reported measures (in men, positive correlations at the level of < .1). Table 2 presents the correlation coefficients for the study.
Table 2
Correlation coefficients between variables for women and men
Next, we investigated H1: that mothers were more responsive than fathers according to both self-reported and observational scales. Table 3 presents the results of a dependent samples t-test for differences in mean values of study variables between women and men. Women scored higher than men on parental responsiveness measured with PRS. However, there were no significant differences between mothers and fathers in responsiveness measured with the observational scale.
Table 3
Mean scores and standard deviations (SD) and results of t-test with Cohen’s d effect size estimates for differences between women and men
To test the hypotheses about predictors of parental responsiveness (H2, H3, H4), we conducted APIM analyses. These results are presented in Table 4. For women’s sensitivity toward their child measured during the free play procedure, there was a positive actor effect of empathic concern and a positive partner effect of empathic concern. For women’s parental sensitivity, there was also a negative partner effect of perspective taking; the negative partner effect of personal distress was on the verge of statistical significance.
Table 4
Results of the actor-partner interdependence models with standardized coefficient estimates
For men’s sensitivity toward their child, there was a positive actor effect of empathic concern, a negative actor effect of personal distress, and a positive actor effect of relationship satisfaction; the negative actor effect of attachment anxiety was on the verge of statistical significance.
For women’s cooperation during the interaction with their child, there was a positive actor effect of empathic concern, a negative partner effect of perspective taking, and a positive partner effect of empathic concern that was on the verge of statistical significance.
For men’s cooperation during the interaction with their child, there was a positive actor effect of empathic concern, a negative actor effect of personal distress, and a positive actor effect of relationship satisfaction.
For women’s parental responsiveness (measured with the subjective scale of the PRS), there was a positive actor effect of empathic concern, a negative actor effect of attachment avoidance, and a positive actor effect of attachment anxiety that was on the verge of statistical significance.
For men’s parental responsiveness (measured with the PRS), there were positive actor and partner effects of empathic concern. The negative actor effect of personal distress and the negative partner effect of attachment avoidance were on the verge of statistical significance. Table 2 shows also the correlations between variables. Empathic concern was correlated positively with all responsiveness scales in both women and men. Moreover, in women, self-reported responsiveness was positively correlated with perspective taking and negatively with attachment avoidance. In men, there was a negative correlation between attachment avoidance and sensitivity. Furthermore, their satisfaction with their romantic relationship with the child’s mother was positively correlated with both aspects of responsiveness measured with observational scale for sensitivity and cooperation. Hypotheses H2, H3 and H4 for both women and men were partially confirmed. Furthermore, the partner effect of some parental predictors was confirmed. Moreover, the father’s self-reported responsiveness was correlated with the mother’s responsiveness (measured using both self-reported and observational methods).
DISCUSSION
This research showed that parental responsiveness toward one’s own child is a complex construct that is affected by a variety of factors. At the individual level, measures of responsiveness (self-report and observational) were not congruent and probably depend on other variables. However, in couples, there were positive correlations in three aspects of observed parental responsiveness: sensitivity, declared parental responsiveness, and relationship satisfaction. It is surprising that both observational dimensions of responsiveness (sensitivity and cooperation) were highly correlated with each other, but only sensitivity was correlated in couples. It is worth mentioning that sensitivity towards one’s own child was higher in women than in men, whereas cooperation was higher in men. Thus, these subscales might reflect maternal or paternal roles, respectively, to greater extents. In contrast, whereas women had higher responsiveness than men measured with the self-report method, both assessments were correlated. These results innovatively broaden the understanding of parental responsiveness and highlight the necessity of not only observing parental behaviors in specific contexts but also including subjective perceptions of responsiveness towards one’s own child.
The first hypothesis (H1) was partially confirmed, because not all aspects of observational responsiveness were higher in women. Indeed, paternal cooperation was higher than maternal cooperation. Mothers and fathers have separate but complementary functions in raising children within the family. Mothers tend to be more actively engaged and responsive to the child’s needs, assuming a more nurturing role, while fathers often take on a protective role (Pakaluk & Price, 2020) and engage in play more often. Furthermore, the distinctions in parental behaviors between mothers and fathers may primarily stem from societal gender roles and social gender stereotypes. This includes the expectations that mothers should be nurturing, caring, and responsible for childcare and household tasks (Crouter et al., 1993; Dufur et al., 2010). Thus it might be that mothers reporting their responsiveness in self-report measures are more affected by these stereotypes than when they are actively engaged with the child. The different socialization experiences of men and women encourage gender-based social differences that are displayed in parenthood (Yaffe, 2023). Indeed, in Poland mothers still play a more central and crucial role in child-rearing (Kaźmierczak & Karasiewicz, 2019).
During the free play procedure, our team observed that mothers displayed more nurturing behaviors, including wiping their child’s saliva, adjusting their clothing, and making sure they were comfortable. These behaviors are usually sensitive, but they can also be intrusive when the baby is playing or focusing on something very interesting. Fathers displayed less sensitivity and more cooperation. It was observed that they very rarely interfered with the child’s play. The results of this research align with the findings summarized by Yaffe (2023) in a systematic review, which indicate that mothers are typically more responsive, accepting, supportive, behaviorally controlling (including monitoring), demanding, and autonomy-granting compared to fathers.
PREDICTORS OF SELF-REPORTED AND OBSERVATIONAL RESPONSIVENESS
Empathy. The hypothesis that higher empathic concern and perspective taking in parents are positively correlated with higher responsiveness to their child for both observational and self-assessed measures (H2) was partially confirmed. This study revealed, for both mothers and fathers, that an individual’s dispositional empathy is connected with their being more responsive. A previous study found that more empathic individuals are more likely to form and maintain close relationships. This may be because empathic individuals are better able to understand and respond to the emotional needs of their partners, which is an important aspect of building and maintaining a healthy relationship (Sened et al., 2017). This is related to relationship satisfaction, trust, and stability.
Empathic concern was a universal predictor of every dimension of parental responsiveness in both mothers and fathers, and also displayed an effect on partners. The higher the empathic concern was, the higher were the sensitivity, cooperation, and self-report responsiveness in both mothers and fathers. Moreover, men’s higher empathic concern was related to sensitivity toward the child in women, and women’s higher empathic concern was related to higher self-report responsiveness in men. Effective emotional regulation is crucial for higher levels of sensitive responsiveness (Eisenberg & Eggum, 2009). Empathic reactions are promoted by high emotional regulation, which facilitates setting psychological boundaries between the self and others. Parents with higher levels of empathic concern will be better at regulating their emotions despite the high level of arousal caused by different children’s behaviors, and their neurologically based self-regulatory processing will facilitate empathic responses (Eisenberg & Eggum, 2009). Thus, partners who score higher in empathic concern might be more supportive towards each other during caregiving and coparenting, even in the presence of higher arousal (Kaźmierczak et al., 2022), which might explain partner effects of this empathic dimension in the present study.
Only the father’s, but not the mother’s, perspective taking was a predictor of the mother’s sensitivity and cooperation. When the father scored lower in perspective taking, the mother was more sensitive and cooperative with her child. This discrepancy might suggest that in the first months of a child’s life, the mother, as the primary caregiver, feels that she should provide what the father cannot. Indeed, previous studies revealed that mothers and fathers play distinct but complementary roles. Mothers are more often present and responsive to the child’s needs and fathers are more protective of their family members (Pakaluk & Price, 2020). However, future studies on responsiveness in both parents should focus on these differences to provide an extensive explanation.
Higher personal distress was a significant predictor of lower sensitivity and lower cooperation only in men. Personal distress can be understood as self-oriented empathy. Observing a child’s negative emotions can induce overarousal, thereby promoting self-focus and the desire to alleviate one’s own discomfort, rather than that of the child (Eisenberg & Eggum, 2009). In the case of young fathers, empathy plays a dual role. It impacts their personal capacity to manage negative emotions and also shapes the dynamics of the relationship after the birth of the child, facilitating the transition to parenthood (Kaźmierczak, 2015). Mature empathy mechanisms allow parents to regulate negative emotions more effectively and potentially come to terms more easily with the occurrence of certain challenges in the process of undergoing changes (Verhofstadt et al., 2016).
The father’s caregiving behaviors may be guided by the mother by encouragement or by restrictions (in the case of maternal gatekeeping; Witte et al., 2020). However, this study revealed that the father’s responsiveness judged objectively based on his behavior was not linked with the mother’s dispositional variables, such as empathy or attachment. Nevertheless, the father’s responsiveness judged subjectively (using self-report measures) was connected with the mother’s empathic concern and avoidance in close relationships. A possible explanation for these results can be found in the biological basis of arousal. It may be that men who display lower levels of arousal in caregiving situations also have less insight into others’ emotional states and greater difficulties with perspective taking. Women, who may have a higher level of arousal in situations subject to social judgment, are more focused on fulfilling the child’s needs (Eisenberg & Eggum, 2009).
Couples with high levels of empathy have more positive relationships than those with lower levels of empathy, and individuals in relationships with partners who are highly empathic report greater well-being and life satisfaction (Sened et al., 2017). Partners with similar levels of empathy tend to share more understanding and will likely communicate better (Sened et al., 2017). However, it is worth considering that empathy is a multi-faceted construct, and it is possible that partners may have different levels of empathy in different areas.
Attachment. In mothers the hypothesis that higher attachment avoidance in a parent is linked with lower parental responsiveness (H3) was confirmed only regarding self-assessed measures. According to previous studies, parental responsiveness, measured with a self-report method, is connected with attachment avoidance in close relationships – but only in women. It should be underlined that as self-report is a subjective method, it shows how mothers perceive their own responsiveness. It is likely that higher levels of avoidance in close relationships may be linked to mothers’ perceptions of their availability to receive and react adequately to their child’s signals. However, this was not reflected in the observational measurement. It may be that mothers with higher avoidance assess their competences more rigorously. Moreover, avoidant mothers are less confident with their abilities and, as other studies have revealed, they report more shame when they are caregiving without their partners, compared to when they are coparenting (Kerr et al., 2021). The part of the third hypothesis (H3) pertaining to anxiety in attachment was not confirmed for either mothers or fathers, and this was the case for both observational and self-reported measures. Anxiety did not significantly influence parental responsiveness towards infants.
However, in fathers, the hypothesis that higher attachment avoidance in a parent is linked with lower parental responsiveness (H3) was confirmed with regard to observational measures. In fathers, higher avoidance in close relationships was connected with lower sensitivity measured with the observational scale. This is a very interesting result that should be expanded in future research. Studies have found that parents with a history of insecure attachment tend to be less sensitive and responsive to their children’s needs and signals. These parents may also be more likely to use controlling and punitive strategies in their parenting, which can interfere with the development of a secure attachment between the parent and child (Moss et al., 2004). It is worth pointing out that not all attachment-avoidant parents are unresponsive, and not all unresponsive parents are avoidant, as parenting stress, trauma, and even certain environmental factors can lead to attachment avoidance behaviors in parents, independent of their childhood experiences. This study showed that the links between attachment and parenting behaviors are complex, and this topic should be further explored.
Relationship satisfaction. The hypothesis that higher satisfaction in partners is connected with higher parental responsiveness (H4) was confirmed for fathers for both observational measures. The greater the relationship satisfaction in fathers, the higher was their sensitivity and cooperation toward their own child. This result suggests that, for men, marital satisfaction (or satisfaction in the relationship with the child’s mother) is an important factor for the relationship with the child. Previous research revealed that higher marital satisfaction was correlated with higher parental satisfaction (Yoo, 2020), and it has been found to have a positive impact on the relationship with one’s own child (Kwok et al., 2015). Moreover, marital difficulties result in greater reduction of parental involvement in fathers than in mothers (Gao et al., 2019), and this suggests that relational variables affect men more strongly.
Studying parental sensitive responses and cooperation with ongoing behaviors is crucial given the benefits for children. Undoubtedly, parental responsiveness can help children feel loved, supported, and valued, which can promote their social, emotional, and cognitive development. Indeed, a child having a positive relationship with their parents helps them be more emotionally secure, confident, and capable of forming healthy relationships. Conversely, children who have a negative relationship with parents may be more prone to emotional and behavioral problems (Bakermans-Kranenburg et al., 2003; Cross et al., 2021).
Even if parental responsiveness has been studied by many researchers, there is still a lack of studies integrating the evaluation of this construct with the use of both observational and self-report scales. In the observational scales, which are as objective as possible, there is a situational context that is also included in the measurement. However, observational scales do not include individual dispositions, which are present in self-report scales. As has been shown in this research, it is very important to study this topic from different perspectives, because there are individual differences in parental responsiveness that depend on the tools used to measure it.
CONCLUSIONS
The present research shows that parental responsiveness towards one’s own child is a behavior determined by many factors. Moreover, one’s own judgment of this aspect differs from objectively evaluated components of this behavior. Individual differences in parents are often overlooked in research regarding parental responsiveness and are rarely studied using different perspectives (objective and subjective). However, some limitations should be emphasized. This study faces the common limitation of the sample consisting of volunteers: parents who volunteer may be more interested in parenting than those who do not – subjective parental responsiveness scores were high, whereas sensitivity and cooperation scores had distributions close to normal. This suggests that parenting is such an important role that every engaged parent wants to be (or shows themselves to be) as responsive as possible. Moreover, parents who volunteer for this type of research may be looking for feedback about their children’s health and their behaviors toward them. However, the good health of the child was one of the inclusion criteria and was checked by a diagnosAll measurements were carried out during a single visit, which limits the interpretation of the results. However, a multimethod approach was implemented, which constitutes a major strength of the study. The observational procedure of free play between the parent and child allowed us to make measurements based on realistic interactions that emerged in a situational context, even if the context was limited to the laboratory room. Parents could present how they care for their child in a new, unknown situation, which was potentially stressful for both parent and child. Indeed, the present study uniquely combined observational and subjectively measured factors.
It is worth noting that this study was performed with a large sample of triads and included fathers of young children, who are often excluded from research on parental responsiveness, especially toward infants. The inclusion of fathers and the reciprocal influence of mothers and fathers on their responsiveness are innovative and add important context to the research. Our findings suggest the importance of including both parents in analyses of the responsiveness of caregivers.