BACKGROUND
Bulimia nervosa (BN) is a type of eating psychopathology that profoundly affects physical and mental health, primarily for women (Mitchell et al., 2014; Keel & Forney, 2013). The life-time prevalence of BN in women is 1.8% (Galmiche et al., 2019) with full-blown eating disorders manifested between 18 and 21 years of age (Hudson et al., 2007). The prevalence of BN and other eating disorders among college/university women is a major source of concern for clinical psychologists and educators (NEDA, 2013). The current research therefore examined BN in women and for women attending college/university. The purpose of the current research was to test the social withdrawal syndrome (SWS) hypothesis of BN, which posits that a coherent set of social withdrawal variables contribute to and maintain BN (Rotenberg et al., 2013). SWS promotes BN because it undermines women’s dietary restraint, receiving social support by close relationships, and receiving clinical treatment (Rotenberg et al., 2013; Rotenberg & Sangha, 2015). Although supportive of the SWS hypothesis, the existing research has limitations and omissions which were addressed by the current research. The research examined bulimic symptoms as a marker of BN.
SUPPORT FOR THE SWS HYPOTHESIS OF BN
The SWS includes components of low trust beliefs in others, high loneliness, and low disclosure to others. In support of the SWS hypothesis, research has shown that bulimic symptoms are associated with loneliness, low trust beliefs in others and low disclosure to others (Rotenberg et al., 2013, 2017). The research further shows that trust beliefs in others negatively predicts changes in bulimic symptoms during adolescence and thus is a probable cause of those symptoms. Also, the longitudinal relationship was mediated by loneliness, thus demonstrating that it is responsible for the relationship between low trust beliefs and bulimic symptoms (Rotenberg & Sangha, 2015).
The current research was designed to redress the following three limitations or omissions in the research literature. First, research has not specifically examined whether bulimic symptoms are associated with affective withdrawal as predicted by the SWS hypothesis. The research shows that loneliness is associated with bulimic symptoms, but loneliness has been assessed as a cognitive construct (i.e., dissatisfaction with the quality or quantity of relationships) rather than as affect per se. Researchers have found that bulimic symptoms are associated with an array of negative emotions and corresponding emotional dysregulation (Lavender et al., 2015) but the research has not examined affective withdrawal separately. According to the SWS hypothesis, affective withdrawal should be associated with bulimic symptoms. According to this hypothesis, affective withdrawal promotes BN because it undermines women’s dietary restraint, which causes a vicious cycle of food consumption and dieting behaviors symptomatic of this type of eating disorder.
Second, according to the SWS hypothesis, women with BN and elevated bulimic symptoms should hold a dysfunctional relationship schema (see Baldwin, 1992) in which they perceive that they lack social connectiveness with others. Research confirms that women with BN and elevated bulimic symptoms show a range of relationships problems. They demonstrate heightened social conflicts, social criticism, self-criticism, avoidance attachment, fear of intimacy, low self-disclosure, and social incompetence (Evans & Wertheim, 2002; Grisset & Norvell, 1992; Pruitt et al., 1992; Reiss & Johnson-Sabine, 1995; Steiger et al., 1999; Tasca & Balfour, 2014). However, the findings do not show whether women with BN or elevated bulimic symptoms hold a dysfunctional relationship schema comprising a perceived lack of social connectiveness. This hypothesis was tested in the current research by engaging women in a lab-based peer interaction situation. This method permitted control over a range of extraneous factors (e.g., social reactions by others) so that women’s perceived lack of connectiveness with others could be accurately assessed. According to the SWS hypothesis, this dysfunctional schema undermines satisfactory peer friendships. This detracts from the support they could receive from peers for coping with the eating disorder and other social problems.
Third, a test of the SWS hypothesis of BN requires that the complete set of measures of social withdrawal function are a coherent (latent) factor which is associated with bulimic symptoms. To date, research has shown only that there are associations between measures of social withdrawal and that those are associated with bulimic symptoms (Rotenberg et al., 2013). This was redressed by the structural equation modeling statistical strategy, which examined the relationship between the latent measure of social withdrawal underlying all measures and testing the relationship between that latent measure and bulimic symptoms.
OVERVIEW OF THE CURRENT STUDY AND HYPOTHESES
Women completed standardized measures of trust beliefs in close others, disclosure, and affective withdrawal. They were engaged in a lab-based interaction with a same gender peer. Their perceived lack of social connectiveness was assessed by their perceptions of that interaction.
It was hypothesized that:
There would be associations between the three measures of social withdrawal (hypothesis 1).
Bulimic symptoms would be associated with affective withdrawal and lack of social connectiveness and negatively associated with trust beliefs in close others and disclosure (hypothesis 2).
As a structural equation modeling test of the SWS hypothesis model, it was expected that there would be a coherent latent factor with paths to the four social withdrawal measures. Also, there would be a path between that latent factor and bulimic symptoms (hypothesis 3).
PARTICIPANTS AND PROCEDURE
PARTICIPANTS
The participants were 88 female undergraduates (Mage = 21 years 6 months, SD = 5 years 3 months, from 18 to 39 years of age) enrolled in a modest size university in the UK. They were solicited by advertisements on campus as an investigation of the factors affecting students getting acquainted. They were offered the potential to win a modest lottery prize for participating. Research of this type is ongoing on the university campus and typically solicits a representative sample of the university population. The university attended by the participants was composed of 75% White and of 25% from other racial backgrounds comprising 16% Asian, 5% Black and 4% Mixed Race. The study was approved by the appropriate institutional ethics committee, and it adhered to American Psychological Association Ethics Guidelines.
MEASURES
Bulimic symptoms. The Stirling Eating Disorder Scales (SEDS) includes the Bulimic Dietary Cognitions (BDC) and Bulimic Dietary Behaviors (BDB) subscales. Each subscale has demonstrated content validity, reliability (α > .83, and test-retest r > .85, p < .001), construct validity and interpretability (Burton et al., 2016; Williams et al., 1994). The BDC and BDB subscales differentiate between individuals diagnosed with BN and those with other eating disorders (Williams et al., 1994). In the current study, the BDC and BDB subscales showed acceptable internal consistency, α = .85, and α = .81, respectively. The two subscales were highly correlated, r(86) = .66, p < .001, and were summed (and averaged) to construct a bulimic symptoms scale. Higher scores denoted greater bulimic symptoms.
An insight into the BN quality of the current sample is provided by a comparison of their bulimic symptoms to those of clinical and other nonclinical samples. Williams et al. (1994) reported that women who were clinically diagnosed with BN had an Ms of 36.75 (SD = 7.70) and 34.54 (SD = 9.80) for BDC and BDB subscales, respectively. They tested a group of women (the control group) without BN or other eating disorders who had Ms of 5.53 (SD = 8.80) and 3.79 (SD = 6.10). for BDC ns and BDB subscales, respectively. The current sample had means = 10.48 (SD = 9.34) and 10.24 (SD = 7.58) for BDC and BDB subscales, respectively. The current sample in the current study had bulimic symptoms that were approximately twice the scores of women in the control and approached the scores of women with BN. The current sample of women may be regarded as having the upper range of bulimic symptoms with some disposed to BN.
Trust beliefs in close others. The Generalized Trust Beliefs Scale–Late Adolescence (GTBS; Randall et al., 2010) assesses late adolescents’ trust beliefs in four close others (mother, father, romantic partner, and peer). The GTBS-LA has shown acceptable internal consistency, α > .80 (Randall et al., 2010) and expected factor structure (Rotenberg et al., 2013). In the current study, the GTBS-LA showed acceptable internal consistency, α = .82. The items were summed (and averaged) to construct a scale. Higher scores denoted greater trust beliefs in close others.
Affective withdrawal. The 16-item UWIST Mood Adjective Checklist assessed 5-point Likert ratings of emotions (Matthews et al., 1990). The UWIST items in this study were subjected to a principal components analysis that yielded 5 factors accounting for 64% of the variance. The second ‘affective withdrawal’ component had an eigen value of 2.50 and accounted for 15.6% of the variance. This affective withdrawal factor had high loadings on the social withdrawal emotions of loneliness (.61), shyness (.60), sadness (.73), upset (.66), and nervousness (.74). The items were summed (and averaged) to construct a scale in which higher scores denoted greater affective withdrawal.
Disclosure. The Opener Scale (Miller et al., 1983) uses a 5-point Likert scale to assess the willingness to disclose 7 intimate topics to a same-sex friend (e.g., my deepest feelings). In the current study, the scale demonstrated acceptable internal consistency, α = .82. The items were summed (and averaged) to yield a disclosure scale. Higher scores denoted greater disclosure.
Social connectiveness. The 8-item self-report scale involves 7-point Likert ratings of the quality of a relationship (Bernieri et al., 1996; Rotenberg et al., 2010). The 4 relevant items were co-operative (reverse scored), unsatisfying, cold, awkward, engrossing (reverse scored), unfocused, unfriendly, and dull. The items were summed and averaged to construct the lack of social connectiveness (LSC) scale. The LSC scale showed acceptable internal consistency, α = .78 with higher scores denoting greater perceived lack of social connectiveness. The scale distribution was skewed, and it was subjected to a log 10 transformation to normalize its distribution.
PROCEDURE
The research was carried out pre-COVID in 2016. Each participant was individually administered by an experimenter the standardized scales of bulimic symptoms, trust beliefs in close others, and disclosure. She was then engaged in a conversation with a female student (a confederate) for the expressed purpose of “getting acquainted with her”. The participant selected a topic from the disclosure scale, providing a disclosure on the topic. The partner did the same and chose to disclose the likes/dislikes topic (a middle ranked intimacy topic). The experimenter then stated that the study had to end because of shortness of time. The participant was asked to complete ratings of her experiences of the interaction which included the LSC scale. Preliminary analyses showed that the pattern of findings was the same for each of the two conversation partners.
The data are available on the Open Science Framework, https://osf.io/zwdt3/?view_only=9f513e3b9ec84e32879c1b4f7c7586f9.
RESULTS
CORRELATIONS BETWEEN THE MEASURES
The correlations (with Ms and SDs) are shown in Table 1. The hypothesized associations between the measures of social withdrawal were found (hypothesis 1). Affective withdrawal was correlated with lack of social connectedness. Trust beliefs in close others was correlated with disclosure. Trust beliefs in close others and disclosure were negatively correlated with social withdrawal and lack of social connectiveness. As hypothesized (hypothesis 2), bulimic symptoms were: (a) correlated with affective withdrawal and lack of social connectiveness, and (b) negatively correlated with trust beliefs in close others and disclosure.
Table 1
Correlations between the measures (with Ms and SDs)
STRUCTURAL EQUATION MODELING ANALYSIS
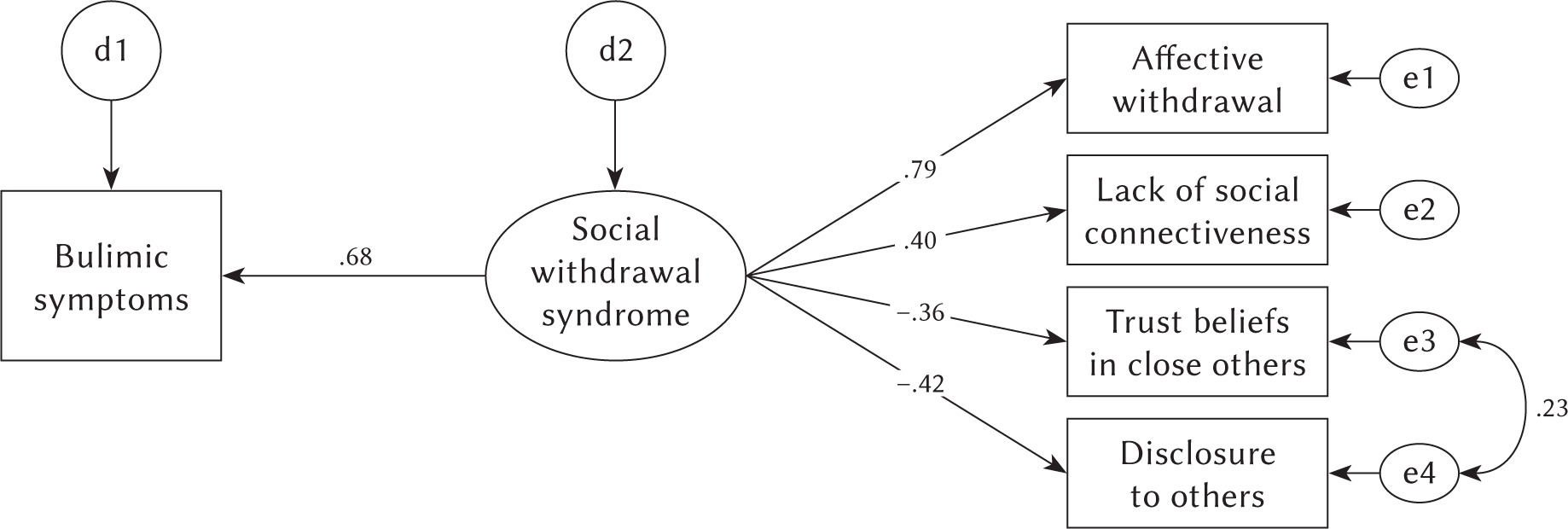
A structural equation modeling (SEM) analysis tested the adequacy of the SWS model (shown in Figure 1). It yielded χ2(4) = 4.08, p = .400, normed fit index (NFI) = .94, comparative fit index (CFI) = 1.00, and a root mean square error of approximation (RMSEA) = .015. There was one covariance between two error terms (designated as es in Figure 1). There are disturbances as estimates of error for both bulimic symptoms and social withdrawal syndrome (designated as ds in Figure 1). All the paths attained significance at p < .05. The model was a good fit of the data and yielded a non-significant χ2, NFI and CFI > .90, RMSEA < .060 (Hu & Bentler, 1999). Support was found for the hypothesized model (hypothesis 3). As expected, the latent factor social withdrawal syndrome factor had paths: (a) to affective withdrawal and lack of social connectiveness measures and (b) (negatively) to trust beliefs in close others and disclosure. Also, there was a path from that social withdrawal syndrome factor to bulimic symptoms.
DISCUSSION
The study yielded support for all three hypotheses. As expected, there were associations between the measures of social withdrawal. Furthermore, the measures of social withdrawal were associated individually with bulimic symptoms. This corroborated the findings that bulimic symptoms are negatively associated with trust beliefs in close others and disclosure (Rotenberg et al., 2013; Rotenberg & Sangha, 2015). The findings further showed that bulimic symptoms were associated with affective withdrawal and lack of social connectiveness. The structural equation analysis yielded support for the social withdrawal syndrome model. There was a coherent latent social withdrawal factor with paths to all four social withdrawal measures and a path between it and bulimic symptoms.
The observed association between bulimic symptoms and affective withdrawal is consistent with the research which shows that an array of negative emotion and corresponding emotional dysregulation are associated with BN and elevated bulimic symptoms (e.g., Lavender et al., 2015). The current findings support the conclusion that a specific form of negative affect – affective withdrawal – plays a separate role in BN. Specifically, this type of affect undermines dietary restraint, which contributes to the vicious cyclic pattern of food consumption and dieting behaviors symptomatic of this type of eating disorder.
The current findings provide further insights into the psychosocial problems of women who have elevated bulimic symptoms and are at risk for BN. Their perception that they lack social connectiveness would undermine establishing satisfying peer relationships. As a consequence, the women would be unlikely to solicit social support from peer friends for assistance in their eating disorder and other psychosocial problems. The unwillingness to disclose personal information to close others, including eating behavior (accompanied by other aspects of social withdrawal) would undermine the detection of their eating disorder and the likelihood that they would receive clinical treatment (see Rotenberg et al., 2013, 2017). Specifically, they would be unlikely to reveal their BN cognitions and behavior to others and thus receive clinical treatment for them.
Based on current findings it would be worthwhile to include measures of social withdrawal in a program for detecting eating disorders in women (e.g., Smink et al., 2012), particularly those in college/university (NEDA, 2013). The combination of elevated bulimic symptoms and elevated social withdrawal measures would identify women who are at highest risk. They would be prone to BN but would be unlikely to: (a) establish close relationships which would provide social support for coping the eating disorder and social problems; (b) disclose their eating problems to others and (c) because of the latter receive clinical treatment. These women would comprise those with ‘hidden’ eating disorders and who require screening in order to be identified with the disorder and receive clinical treatment for it.
The current research is limited because it is cross-sectional in design. In future, longitudinal research should be carried out to examine whether a latent social withdrawal syndrome factor is a probable cause of bulimic symptoms. Furthermore, researchers should test the SWS hypothesis for men because they also experience BN, although less frequently than women. Also, the research should examine whether women who have been clinically diagnosed with BN show the pattern indicative of the SWS rather than women who do not have any evidence for BN or other eating disorders. Finally, in future researchers could examine the adequacy of the SWS hypothesis to account for other eating disorders, such as anorexia nervosa.