BACKGROUND
Premenstrual dysphoric disorder (PMDD) is a severe mood-related condition affecting 3-8% of women of reproductive age. It is characterized by affective, cognitive, and physical symptoms that occur during the luteal phase of the menstrual cycle and resolve shortly after menstruation. PMDD is classified as a mental disorder in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5; APA, 2013) and has an International Classification of Diseases, 11th Revision (ICD-11; WHO, 2019) diagnostic code, underscoring its recognition as a legitimate medical condition. Despite this, many women remain undiagnosed or misdiagnosed. The theoretical origins of PMDD date back to the early 20th century (Mason-Hohl, 1940). The distinction between premenstrual syndrome (PMS) and PMDD is primarily based on the severity of symptoms, with PMDD presenting with significant impairment in social, occupational, or relational functioning. The exact pathophysiology of PMDD is not well understood and clarified. Etiology is considered multi-factorial. Research data have shown abnormalities in the hypothalamus-pituitary-ovary axis and brain serotonergic system in this patient population (Inoue et al., 2007; Protopopescu et al., 2008). Key factors include hormonal, genetic, environmental and psychological influences. Fluctuations in sex hormones, particularly estrogen and progesterone, are implicated. The altered sensitivity of the serotonergic system to hormonal changes is considered central to the pathogenesis (Inoue et al., 2007; Protopopescu et al., 2008). In recent years, research has focused on identifying PMDD-specific biomarkers. Studies have continued to highlight the importance of the sensitivity of the serotonergic system to hormonal fluctuations, supporting the theory that PMDD is linked to an abnormal interaction between estrogen, progesterone, and the serotonin neurotransmitter system. Gingnell et al. (2013) explored the role of hormone modulation on functional brain connectivity, identifying specific alterations in the response of the serotonergic system in women with PMDD compared to those without the disorder. Researchers have found potential genetic differences that could make some women more likely to develop this disorder. This could lead to personalized therapies tailored to individual genetic profiles. Huo et al. (2007) demonstrated the association between genetic variations in serotonin receptor genes and PMDD, and they suggested that specific variants may play a role in individual vulnerability to PMDD. Anxiety, depression, and other mood disorders can exacerbate PMDD symptoms. Stress is also an important factor. Lifestyles and socioeconomic factors can affect the manifestation of symptoms.
Here are the diagnostic criteria for PMDD according to the DSM-5 (APA, 2013):
In the majority of menstrual cycles over the past year, at least five symptoms must be present in the final week before the onset of menses, start to improve within a few days after the onset of menses, and become minimal or absent in the following week. At least one of the symptoms must be one of the following:
Markedly depressed mood, feelings of hopelessness, or self-deprecating thoughts.
Marked anxiety, tension, or feeling keyed up or on edge.
Marked affective lability (e.g., mood swings, feeling suddenly sad or tearful, or increased sensitivity to rejection).
Marked irritability or anger or increased interpersonal conflicts.
One or more of the following symptoms must additionally be present, to reach a total of five symptoms when combined with those above:
Decreased interest in usual activities (e.g., work, school, friends, hobbies).
Difficulty in concentration.
Lethargy (e.g., fatigue, marked lack of energy).
Marked change in appetite, overeating, or specific food cravings.
Hypersomnia or insomnia.
A sense of being overwhelmed or out of control.
Physical symptoms such as breast tenderness, joint or muscle pain, a sensation of bloating, or weight gain.
The symptoms are associated with clinically significant distress or interference with work, school, usual social activities, or relationships (e.g., avoidance of social activities, decreased productivity and efficiency at work or school).
The disturbance is not merely an exacerbation of the symptoms of another disorder, such as major depressive disorder, panic disorder, persistent depressive disorder (dysthymia), or a personality disorder (although it may co-occur with any of these disorders).
Criterion A must be confirmed by daily prospective ratings during at least two symptomatic cycles. The diagnosis may be provisionally made before this confirmation.
The symptoms are not attributable to the physiological effects of a substance (e.g., a drug of abuse, a medication, or other treatment) or another medical condition (e.g., hyperthyroidism).
Halbreich et al. (2003) reported that approximately 3-8% of women of reproductive age meet the diagnostic criteria for PMDD, but according to other studies (Hartlage et al., 2012), the prevalence may vary slightly depending on the diagnostic criteria used and the assessment methods. Some studies have reported that 5-10% of women of reproductive age may experience significant symptoms of PMDD. Furthermore, PMDD has been observed in women from various cultures and geographical regions, but its prevalence appears to be relatively uniform globally, with variations that may reflect cultural differences in the perception and reporting of symptoms. Hantsoo and Epperson (2015) emphasized that PMDD is recognized worldwide and does not appear to be limited to specific ethnic or cultural groups. However, recognition and diagnosis may vary depending on local clinical practices and awareness of the disorder. The disorder is associated with an increased risk of other psychiatric conditions, including major depression and anxiety. Hartlage et al. (2012) highlighted that women with PMDD have a significantly lower quality of life compared to those without the disorder and often require prolonged medical and psychological treatment.
Treatment of PMDD can be multimodal and includes drug or hormone therapies and non-pharmacological treatment (Hantsoo & Epperson, 2015; Yonkers et al., 2008). Cognitive behavioral therapy (CBT) can help manage psychological symptoms, and lifestyle modifications such as diet, regular exercise, and stress management techniques can alleviate symptoms. In severe cases, the use of gonadotropin-releasing hormone (GnRH) agonists may be considered to induce a temporary menopausal state. The International Association for Premenstrual Disorders (IAPMD) provided a review on treatment guidelines.
The COVID-19 pandemic introduced significant psychosocial stressors that may have exacerbated underlying or subclinical conditions. The psychological effects of lockdown conditions, including isolation, disrupted routines, and increased anxiety, may have intensified premenstrual symptomatology in susceptible individuals and affected the menstrual cycle as well as the depressive symptoms and sleep (Polese et al., 2024). However, the relationship between pandemic stress and menstrual-related mental health symptoms remains under-investigated, particularly in the Italian context.
The prevalence of PMDD in Italy is estimated to be similar to international figures, with about 3-8% of women of reproductive age affected by this condition. However, specific large-scale data for Italy are not widely available. According to some studies conducted on Italian samples, a significant percentage of women report premenstrual symptoms that may be associated with PMDD, even if not all meet the full diagnostic criteria. A study published in 2022 reported that about 77% of the women surveyed suffer from premenstrual symptoms, and a significant portion could meet the diagnostic criteria for PMDD (Hantsoo & Epperson, 2015; Hantsoo et al., 2022; Yankers et al., 2008). In Italy, as elsewhere, risk factors for PMDD include a family history of mood disorders, high stress, and challenging living conditions. The COVID-19 pandemic has been an additional stressor that may have exacerbated premenstrual symptomatology, increasing the number of diagnoses or the severity of symptoms among Italian women. Women with PMDD in Italy may be more likely to suffer from other psychological conditions, such as depression and anxiety, a trend observed in international studies and reflected in the Italian context. Awareness of PMDD among the general population and healthcare professionals in Italy remains relatively low, which can lead to underdiagnosis of the disorder. This issue is recognized globally but is particularly relevant in countries where health education on these topics is not widely disseminated. Many Italian women may not receive an accurate diagnosis of PMDD due to a lack of specific knowledge about the disorder, on the part of both patients and physicians. This leads to an underestimation of the true prevalence of PMDD in the country.
This research aimed to examine how the COVID-19 quarantine affected, or continues to affect, the premenstrual period in Italian women. The quarantine condition has in fact influenced our daily life with consequent psychological repercussions. It is therefore important to determine whether this situation has also influenced the psychological state in proximity to the menstrual cycle.
This study aimed to explore the prevalence of psychological symptoms compatible with DSM-5 PMDD criteria during the COVID-19 quarantine among Italian women. We did not attempt to diagnose PMDD clinically, as the methodology does not include prospective symptom monitoring or validated instruments. Rather, the study offers descriptive insight into symptom reporting patterns during a unique and stressful public health context.
PARTICIPANTS AND PROCEDURE
We conducted a cross-sectional, anonymous online survey in May 2020 using Google Forms. The survey was disseminated through social media platforms and email. Inclusion criteria included identifying as female, being of reproductive age (18-50), having regular menstrual cycles, and living in Italy during the COVID-19 lockdown. A description of the study participants was provided on the first page of the form, including information on the purpose of the questionnaire and how to participate. In the explanatory text, guidelines on the research, measures to protect personally identifiable information, and the scope of use of the collected data were described (GDPR 2016/679). Participants were presented with an informed consent form based on Article 9 of the Italian Psychologists’ Code of Ethics. Given the anonymity of the survey and absence of sensitive data collection, and the independence of the research group, the study was not submitted for formal ethics committee approval. The online survey was designed so that only those who had read all explanations and agreed to voluntarily participate in the survey could start it. The survey included 34 items: 14 based on DSM-5 PMDD symptom criteria (adapted into yes/no questions), and additional items assessing sociodemographic variables (age, region, BMI, education, menstrual history). No validated psychometric scales were used because, for example, the Premenstrual Symptoms Screening Tool (PSST) was validated in Italy only in 2021. The tool was constructed for descriptive exploratory purposes using the symptoms-oriented clinical interview method but was not validated (Table 1). This study employed a convenience sample, as the primary aim was to explore symptom patterns during a unique historical period – the first nationwide lockdown in Italy due to the COVID-19 pandemic. Given the exceptional and time-limited circumstances, it was not feasible to perform a priori sample size calculation or recruit a probabilistic sample. Therefore, all respondents who consented to participate during the data collection window were included. Descriptive statistics were calculated for demographic data. Frequencies and percentages were used to report symptom prevalence. A conservative approximation of symptom clusters consistent with DSM-5 PMDD criteria was used to estimate the proportion of participants who might meet criteria under ideal assessment conditions. Pearson correlations and chi-square tests explored associations between symptom reporting and demographic/clinical variables. IBM SPSS version 20 was used.
RESULTS
The study included 109 women (mean age = 35.89 years, SD = 6.00, range 18-51). Participants were mostly from Southern Italy, with 45 women (41.3%) residing there, 33 (30.3%) from the Center, 11 (10.1%) from the North, and 4 (3.7%) from abroad. Educationally, 68 women (62.4%) held at least a university degree, while 21 (19.3%) had completed high school. The mean body mass index (BMI) was 23.06 (range 17.63-38.28; median 22.27), and the age at menarche ranged from 9 to 15 years, with a median of 12.
Most participants reported regular menstrual cycles (n = 86; 78.9%), typically lasting between 25 and 36 days (n = 90; 82.6%), and more than half had no history of pregnancy (n = 61; 55.9%). Only a small proportion reported a prior psychiatric diagnosis (n = 8; 7.3%) or a previous diagnosis of PMDD (n = 2; 1.8%), although a substantial number had previously sought psychological consultation (n = 41; 37.6%). During the COVID-19 quarantine, 84 participants (77.1%) reported experiencing premenstrual symptoms, highlighting the potential influence of pandemic-related stress on menstrual health.
Table 1
Symptoms-oriented clinical interview
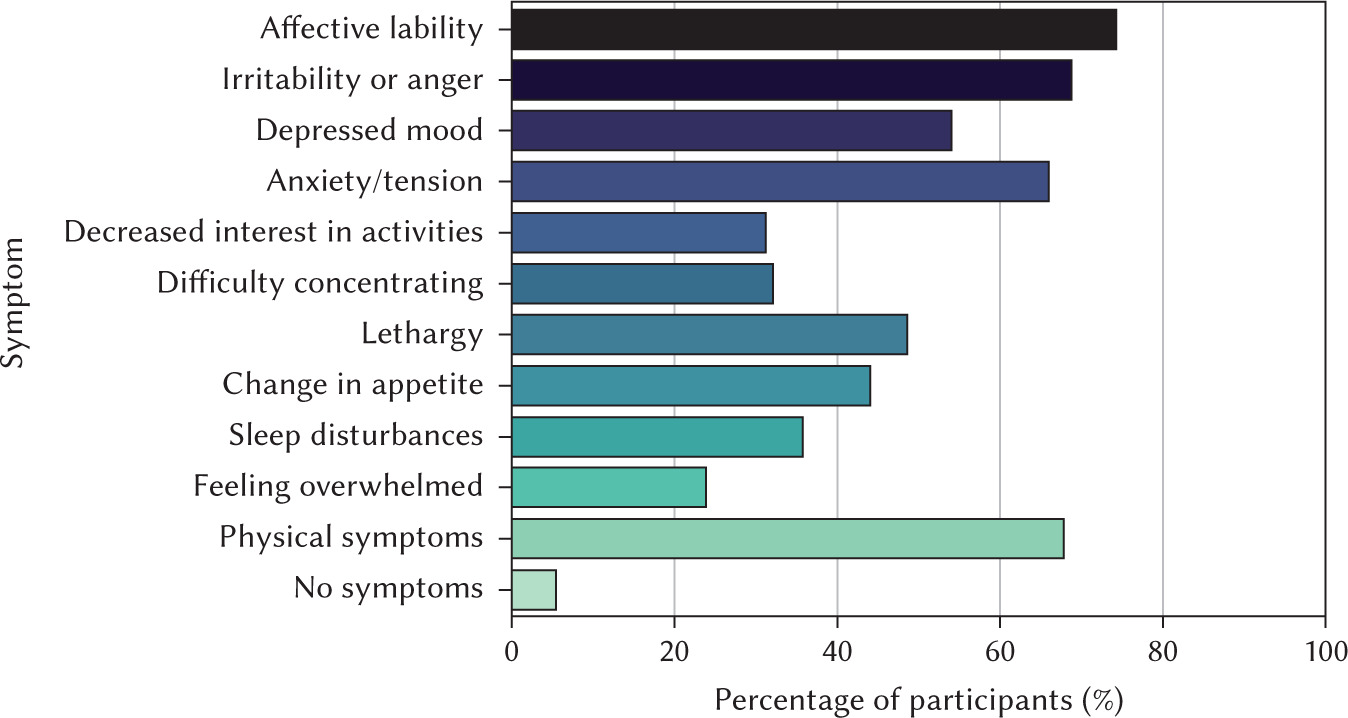
Symptom prevalence based on DSM-5-aligned criteria revealed that affective lability was most frequently reported (n = 81; 74.3%), followed by irritability or anger (n = 75; 68.8%), anxiety or tension (n = 72; 66.1%), physical symptoms (n = 74; 67.9%), depressed mood (n = 59; 54.1%), lethargy (n = 53; 48.6%), appetite changes (n = 48; 44.0%), sleep disturbances (n = 39; 35.8%), and feeling overwhelmed (n = 26; 23.9%), whereas only 6 women (5.5%) reported no symptoms (Figure 1). Notably, 40 participants (36.7%) exhibited symptoms consistent with PMDD, indicating a clinically significant prevalence of self-reported premenstrual mood symptoms in this sample.
No significant correlations were found between symptom frequency and age or BMI.
Of the 109 women, 69 (63.3%) reported experiencing these symptoms across multiple cycles, and 58 (53.2%) reported that the symptoms became more severe during quarantine.
Using DSM-5 criteria, we estimated that approximately 36.7% (40/109) of participants could potentially meet the diagnostic threshold for PMDD, having reported at least 5 symptoms, including one from the core affective group. These findings should be interpreted as self-reported symptom clusters consistent with DSM-5 criteria for PMDD, based on a retrospective, non-validated assessment, and not as a formal clinical diagnosis. Meta-analytic estimates based on prospective confirmation place point prevalence substantially lower (approximately 3.2% overall and 1.6% in community samples), suggesting that retrospective checklist methods may inflate provisional prevalence estimates.
No significant correlations were found between age or BMI and symptom severity (Pearson’s r < .20). A significant association was observed between self-reported history of psychological vulnerability and increased symptom severity during quarantine (p = .042) suggesting prior psychological vulnerability may be a contributing factor.
From the data analysis, a high percentage of the sample can endorse symptom clusters consistent with DSM-5 criteria under retrospective, non-validated assessment, so meet the diagnostic criteria for the diagnosis of PMDD (Table 1). Limitations include its cross-sectional design, potential recall and selection bias, lack of clinical verification, and small convenience sample.
These findings are consistent with recent research demonstrating that the COVID-19 pandemic was associated with heightened premenstrual symptomatology. Pandemic-related stress, lifestyle changes, and health-related anxiety have been identified as factors contributing to both premenstrual and menopausal symptoms, including PMDD, emphasizing the need for heightened clinical awareness and targeted interventions to support women’s mental health during periods of elevated psychosocial stress (Polese et al., 2024).
CONCLUSIONS
This exploratory study suggests that a substantial number of women reported symptoms consistent with PMDD criteria during the COVID-19 lockdown. However, the results must be interpreted cautiously. These findings reflect self-reported symptom clusters consistent with DSM-5 criteria under retrospective, non-validated assessment, and should not be considered a formal clinical diagnosis. The absence of validated instruments, reliance on retrospective recall, lack of symptom severity grading, and failure to assess general psychological distress limit the study’s diagnostic value.
The results of this study diverge from previous literature, which mostly reported a PMDD prevalence between 3% and 10% (Halbreich et al., 2003; Hart-lage et al., 2012). The stress caused by the pandemic may have had significant repercussions on premenstrual symptomatic manifestations. Administration of the questionnaire during quarantine may be both a strength and a weakness of this research. It also seems likely that PMDD is still underestimated due to poor awareness of this disorder.
Recent findings have shown that COVID-19 phobia is associated with increased psychological and somatic symptoms even in peri-menopausal and post-menopausal women, with higher fear scores correlating with more severe symptom burden (Özberk et al., 2024). These results align with our observations, suggesting that pandemic-related distress may amplify mood-related symptom reporting across reproductive stages.
Without controlling for depression, anxiety, or stress, we cannot isolate menstrual-related patterns. Importantly, the findings may partially reflect the pandemic-related psychological burden rather than cyclical mood pathology. Without controlling for depression, anxiety, or stress, we cannot isolate menstrual-related patterns. Future studies should employ prospective symptom tracking, validated tools, and measures of general psychopathology to better assess the interplay between environmental stress and premenstrual symptoms.
Despite the lack of large-scale specific data, available information suggests that PMDD affects a substantial number of Italian women. Furthermore, the non-parametric analysis suggested that a history of psychological issues is associated with worsening symptoms during quarantine.
The study’s strengths include rapid deployment during a public health emergency and a focus on a relatively understudied area. Limitations include its cross-sectional design, potential recall and selection bias, lack of clinical verification, and small convenience sample, and the use of a yes/no symptom checklist, which may overestimate provisional prevalence compared to prospective daily ratings (e.g., the Daily Record of Severity of Problems – DRSP).
Although not diagnostic, the findings highlight the need to monitor women’s mental health in times of collective stress. Increased attention to menstrual cycle-related distress, especially during crises, may support early identification and intervention.