Background
Intellectual disability, now classified as disorders of intellectual development in ICD-11 (WHO, 2019), is a neurodevelopmental disorder characterized by significant limitations in both intellectual functioning and adaptive behavior, originating during the developmental period (Schalock et al., 2021). The severity of intellectual disability is determined by adaptive functioning, as intellectual quotient (IQ) scores are less reliable, particularly in individuals with profound intellectual disability (ID). A diagnosis requires evidence of deficits in both intellectual and adaptive domains (McKenzie et al., 2016; Schalock et al., 2021).
Within the ICD-11 framework, adaptive behavior refers to the collection of conceptual, social, and practical skills used to function in everyday life (WHO, 2019). The conceptual domain includes skills related to academic learning, memory, language (receptive and expressive), reading, writing, mathematical reasoning, knowledge acquisition, and problem-solving (Tassé et al., 2016). Deficits in these skills significantly impact an individual’s ability to understand and apply academic concepts, communicate effectively, manage information, and navigate cognitive challenges in various settings, including school, work, and community life. Assessment of conceptual adaptive skills should consider age-related expectations and cultural norms and involve multiple sources of information, including standardized assessments, observations, and interviews with caregivers and educators (WHO, 2019; Tassé et al., 2016).
Analysis of these definitions indicates that the assessment of intellectual functioning in individuals with intellectual disability extends beyond a simple IQ evaluation. Intellectual functioning, as understood within the ICD-11 framework (WHO, 2019), is considerably broader than the narrow concept of intelligence or intellectual abilities, yet more specific than the overarching construct of human functioning (Schalock et al., 2021). It encompasses not only cognitive capacities measured by IQ tests but also the ability to apply these abilities in real-world contexts, particularly within the conceptual domain of adaptive behaviors. Therefore, a comprehensive understanding of intellectual functioning emerges only from integrating both diagnostic criteria: IQ levels and the assessment of conceptual adaptive behaviors (WHO, 2019; Schalock et al., 2021; Tassé et al., 2016). This dual approach enables a more accurate depiction of an individual’s cognitive and functional capacities, aligned with developmental expectations and sociocultural contexts.
The most comprehensive and empirically supported framework for understanding cognitive functioning is the Cattell-Horn-Carroll (CHC; see Figure 1) theory of intelligence (McGrew & Evans, 2023; McGrew & Wendling, 2010; Schneider & McGrew, 2018). Due to its hierarchical structure, CHC theory offers a nuanced, multidimensional understanding of cognitive functioning, going beyond the limitations of a single IQ score. It organizes cognitive abilities into three strata – general (Stratum III), broad (Stratum II), and narrow (Stratum I) – thus avoiding the error of equating intellectual functioning with the general intelligence factor (g). Instead, it conceptualizes intellectual functioning as a complex, multilayered construct of interrelated, yet distinct, cognitive domains (Schneider & McGrew, 2018).
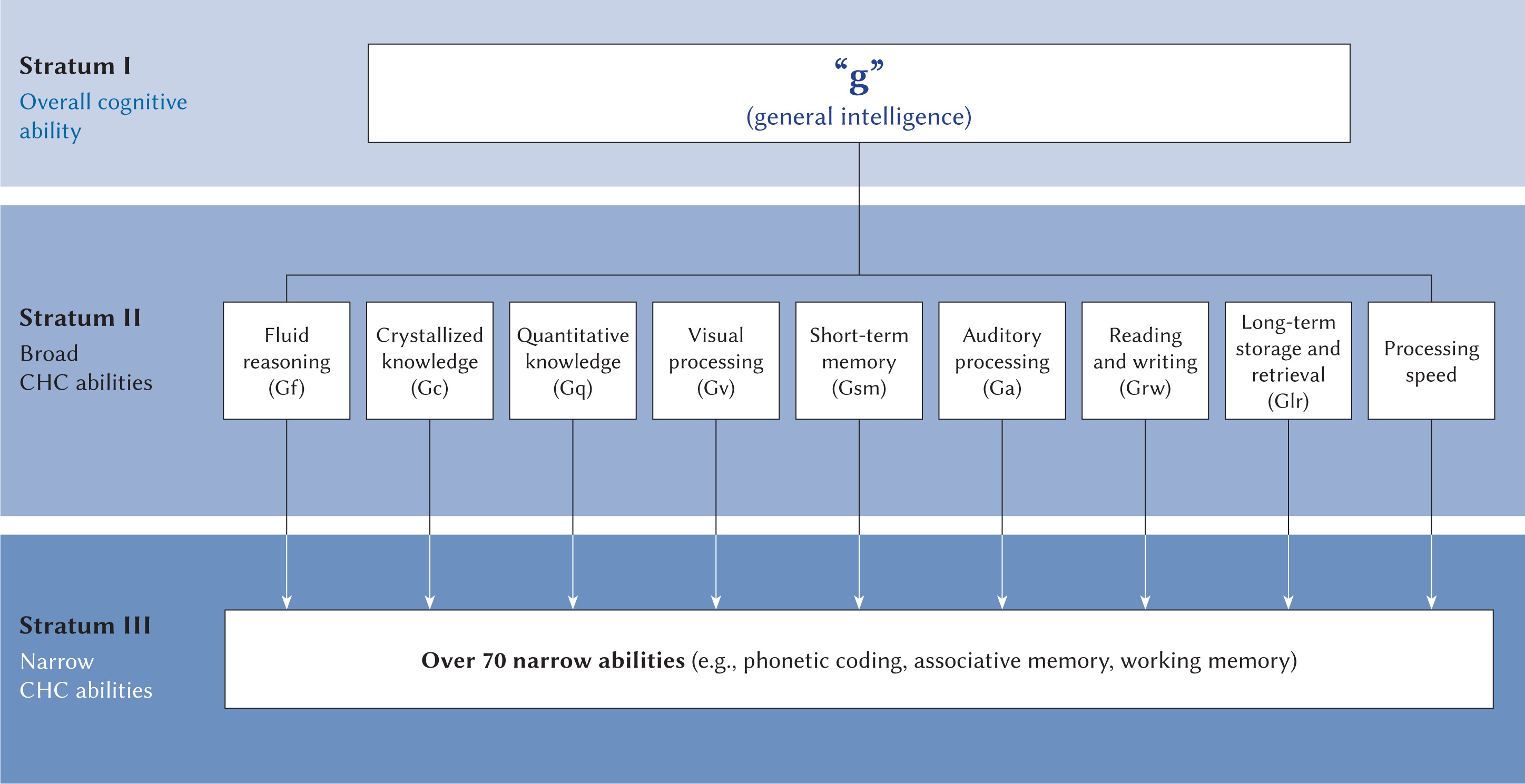
Best practices in IQ assessment include at least six subtests targeting both fluid reasoning (Gf) and crystallized knowledge (Gc), alongside sampling from at least three, and preferably more, CHC broad-stratum abilities (Schalock et al., 2021). However, relying solely on intelligence tests based on the second stratum of the CHC theory is insufficient for a comprehensive evaluation of intellectual functioning in ID. It is essential to also assess additional cognitive processes often situated within the first stratum of CHC theory – for example, language development, associative memory, and communication ability – as these are closely linked to conceptual adaptive behaviors (Schalock et al., 2021). These lower-order cognitive abilities are critical for understanding how individuals apply cognitive resources in daily functioning, particularly in academic and communicative contexts, and thus contribute substantially to diagnostic decisions regarding ID.
Contemporary scholarship increasingly emphasizes that ID should be viewed as a condition rather than a numerical value (Greenspan et al., 2015). The overreliance on fixed IQ thresholds – such as the traditional cut-off at a full-scale IQ of 70 – has been criticized for lacking scientific rigor and for producing false positives and false negatives in diagnostic decisions. As Greenspan et al. (2015) argue, such thresholds offer only an illusion of objectivity and fail to account for measurement error, cultural variation, test obsolescence, and the multidimensional nature of cognitive and adaptive functioning. This perspective aligns with the shift in the ICD-11 (WHO, 2019) and DSM-5 (APA, 2022) toward diagnostic models that prioritize real-world functioning and clinical judgment over rigid psychometric indices. The ethical implications of this shift are considerable, as inappropriate use of numerical cut-offs may unjustly deny individuals access to essential services, supports, and legal protections.
Consequently, the diagnostic framework for ID must incorporate a flexible, evidence-based approach that integrates quantitative data with qualitative assessment of adaptive behavior. As Greenspan et al. (2015) suggest, a sole focus on IQ fails to capture the full range of cognitive challenges, particularly in social and conceptual functioning. Their work supports the principle of intellectual and developmental disability (IDD) equivalence, which recognizes individuals who function adaptively as though they have an ID, even with IQ scores above traditional thresholds. This concept reinforces the need to assess the whole person in context, recognizing that cognitive limitations may manifest in ways not reflected in standardized scores. Ultimately, a rational and ethical diagnostic process must move beyond reductionist classifications and adopt a multidimensional, person-centered model of intellectual functioning.
Given the conceptual and diagnostic complexities outlined above, this article proposes evidence-informed recommendations to support clinicians in the comprehensive assessment of cognitive functioning in individuals with mild ID (MID). These guidelines aim to enhance clinical judgment within the diagnostic process, particularly in alignment with the CHC theory. The recommendations were developed based on recent research aimed at capturing the cognitive functioning profiles of individuals with MID across multiple cognitive domains to inform clinical assessment with evidence-based conclusions. Given the multidimensional nature of intellectual functioning and the limitations of relying solely on global IQ scores, particularly considering recent ICD-11 (WHO, 2019) diagnostic criteria, the proposed framework seeks to support clinicians in further formalizing what has long been best practice in many clinical settings: integrating quantitative psychometric data with qualitative observations of adaptive behavior, contextual information, and developmental history. While such integration has traditionally informed diagnostic reasoning, ICD-11 (WHO, 2019) now formally mandates the inclusion of adaptive functioning in both diagnosis and severity classification. Despite this, in research contexts and some institutional settings, reliance on IQ scores as the sole criterion remains common, underscoring the need for consistent application of multidimensional diagnostic models.
Emphasis is placed on identifying and interpreting cognitive strengths and weaknesses across relevant CHC domains, such as fluid reasoning (Gf), crystallized knowledge (Gc), working memory (Gwm), and long-term retrieval (Glr). By offering structured guidance grounded in contemporary intelligence theory, these recommendations aim to reduce diagnostic ambiguity, ensure consistency across evaluative contexts, and promote a person-centered, ethically sound approach to identifying cognitive strengths and weaknesses in ID.
Foundational principles of cognitive assessment in mild ID
Move beyond global IQ
Reliance on a single full-scale IQ score for diagnostic classification has increasingly been recognized as insufficient (Greenspan et al., 2015; Schalock et al., 2021). Intellectual functioning should be understood as a multidimensional construct encompassing diverse cognitive domains and adaptive capabilities. This broader conceptualization offers a more accurate reflection of real-life challenges and accommodates the heterogeneity observed in individuals with MID (Sajewicz-Radtke et al., 2022).
Incorporate CHC theory framework
The CHC model provides a comprehensive, empirically validated framework for identifying both broad (e.g., Gf, Gc, Gwm) and narrow (e.g., lexical access, phonological processing) cognitive abilities (McGrew et al., 2023; McGrew & Wendling, 2010; Schneider & McGrew, 2018). Applying this model enables precise mapping of individual cognitive strengths and weaknesses and supports coherent interpretation of test data in alignment with real-world demands.
Person-centered evaluation
Assessment practices should integrate categorical diagnostic models with individualized, profile-based interpretations (Schalock et al., 2021). Evaluations should thus be informed by a comprehensive understanding of the individual’s cognitive patterns, learning history, and sociocultural background. A person-centered approach facilitates tailored intervention planning that addresses specific cognitive and adaptive needs rather than applying generalized assumptions based on diagnostic labels.
CHC-informed diagnostic practice
Sample multiple broad abilities
Consistent with CHC theory, assessment should include a representative range of broad cognitive abilities – particularly Gf, Gc, and Gwm – to capture the multidimensionality of cognitive functioning (Schneider & McGrew, 2018). Ideally, clinicians should include additional domains such as quantitative knowledge (Gq) and visual processing (Gv) to construct a comprehensive cognitive profile that is sensitive to individual differences, especially for persons with MID (Sermier Dessemontet et al., 2020; Giuliani & Schenk, 2015; Memisevic & Sinanovic, 2013). Current best practices recommend the inclusion of at least six subtests targeting both Gf and Gc, alongside sampling from three or more CHC broad-stratum abilities (Schalock et al., 2021). This approach increases diagnostic precision and ecological validity of profile interpretation. It also necessitates the use of diagnostic tools that are normed, validated, and adapted for individuals with IDs (Flanagan et al., 2022). Such instruments must be capable of capturing both typical and atypical response patterns while accounting for common limitations in attention, language, and processing speed (Flanagan et al., 2022).
Target functional relevance
Selection of assessment domains should prioritize ecological validity – their demonstrated relevance to daily functioning and adaptive behavior. For example, evaluating quantitative knowledge, verbal reasoning, and phonological processing is critical for identifying deficits in academic skills, self-regulation, and communication. This ensures that cognitive data are interpreted within the context of real-world demands. Functional relevance should also be informed by the developmental, educational, and psychosocial challenges typically encountered by individuals with MID (WHO, 2019). Targeting abilities that predict real-world outcomes – such as planning and inhibition (components of executive functioning), receptive and expressive language, and memory retrieval – enhances the utility of assessment findings. Instruments should simulate everyday problem-solving, communication, and learning contexts to improve both validity and accessibility for this population (Xiaoming, 2010).
Evaluate narrow Stratum I skills
A truly informative cognitive evaluation must also assess Stratum I narrow abilities, which often underpin adaptive behavior (Schalock et al., 2021). These include lexical access, semantic fluency, associative memory, and attentional control – skills central to conceptual adaptive functioning such as expressive language, literacy, and learning-to-learn capacities (Schwartz, 2017; Vandereet et al., 2011). Particular attention should be given to those narrow abilities that underlie reading, writing, and listening comprehension, which are frequently impaired in this population. For example, skills such as phonemic awareness, orthographic processing, and rapid automatic naming are critical subcomponents of reading fluency (Melby-Lervåg et al., 2012). Similarly, auditory processing – including phonological discrimination and auditory short-term memory – supports language acquisition and verbal learning (Gathercole et al., 2008; Jacquemot & Scott, 2006). Long-term storage and retrieval (Glr), especially tasks involving associative memory and meaningful recall, are equally vital for encoding and retrieving conceptual information (Lifshitz et al., 2011). Assessing these abilities provides insights into specific academic or adaptive difficulties, even when broad scores appear within expected ranges. Therefore, a thorough analysis of Stratum I functioning allows clinicians to formulate more precise interventions and strengthens the ecological validity of the diagnostic process (Flanagan et al., 2022).
Clinical judgment and diagnostic integrity
Integrate multi-source data
A critical aspect of diagnosing ID is the integration of multi-source data, synthesizing information from diverse assessment methods. While psychometric tests provide quantitative data on cognitive functioning, they have to be complemented by adaptive behavior scales, clinical observations, and informant reports to provide a holistic view of an individual’s abilities (Greenspan et al., 2015; Schalock et al., 2021). Psychometric tests offer valuable insights into cognitive domains but may not capture the nuanced complexities of adaptive behavior (Tassé et al., 2016). Adaptive behavior scales are essential for evaluating the practical application of cognitive skills in real-world settings. These tools enable clinicians to gauge individuals’ competence in daily living tasks, which are critical to understanding how intellectual deficits manifest in educational, social, and occupational contexts (Schalock et al., 2021). Additionally, clinical observations allow for the assessment of real-time behavior, while informant reports from family members, teachers, or caregivers help contextualize functioning within specific environments (Tassé et al., 2012, 2016). Integrating this information facilitates a comprehensive diagnosis and helps avoid reductive interpretations based solely on isolated test scores.
To clarify how diverse data sources can be systematically integrated into diagnostic decision-making, we propose a model of diagnostic inference (Figure 2). The model illustrates how psychometric indicators (e.g., IQ and CHC-based cognitive profiles), adaptive behavior (based on structured observation and validated rating scales), and contextual data (such as educational background, family support, and cultural context) converge in the formulation of an individualized clinical judgment. This judgment then informs a diagnostic outcome that combines both categorical criteria and profile-based interpretations. Such integration aligns with ICD-11 guidelines and supports tailored, evidence-based recommendations for intervention and support.
Figure 2
Integrated model of diagnostic inference in the assessment of cognitive functioning in individuals with intellectual disability
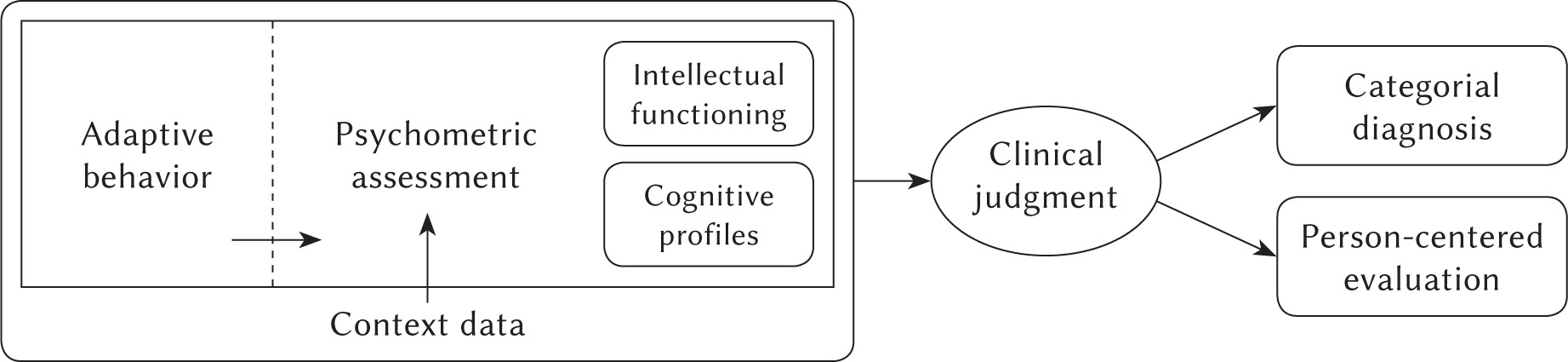
Importantly, the evaluation of adaptive behavior and contextual data should not only inform the dia- gnostic conclusion but also precede and guide the selection of psychometric tools. Understanding the individual’s developmental trajectory, social environment, and functional demands is essential for choosing assessment methods that are valid, relevant, and appropriate for their specific needs and circumstances.
When discrepancies arise between IQ scores and observed adaptive functioning, ICD-11 (WHO, 2019) guidelines prioritize adaptive functioning in determining the severity level of intellectual disability. This reflects the principle that real-world competencies, not abstract cognitive potential alone, dictate the level of support an individual requires. In such cases, adaptive functioning becomes the primary diagnostic anchor. Nonetheless, integrating psychometric data, contextual factors, and clinical insight remains essential, particularly when the diagnostic picture is ambiguous or does not conform neatly to standardized thresholds.
Account for developmental and cultural norms
Accurate assessment of intellectual functioning must consider both developmental and cultural factors, which significantly influence the expression and interpretation of cognitive and adaptive behaviors (Allison & Strydom, 2009; Odom et al., 2009). Developmental norms provide a framework for comparing an individual’s performance to age-appropriate milestones and trajectories, which are essential for diagnostic judgment (Luckasson & Schalock, 2015).
Cultural context is equally important. Cognitive assessments and adaptive behavior scales often contain implicit biases rooted in Western educational and social expectations, potentially leading to misdiagnosis in individuals from non-Western or culturally diverse backgrounds (Allison & Strydom, 2009). For example, language-based assessments may disadvantage individuals whose primary language differs from that used in the assessment or who lack exposure to the academic and cultural norms implicit in certain assessments (Schalock et al., 2021). While the application of age norms is standard in clinical settings, culturally validated norms remain limited or unavailable in many contexts. As such, the recommendation to use culturally sensitive frameworks should be considered aspirational and context-dependent. Clinicians are encouraged to adapt testing procedures when feasible and to interpret results through a culturally responsive lens, while also being mindful of the psychometric constraints and risk of overgeneralization in the absence of robust normative data. This approach enhances diagnostic accuracy and promotes a more inclusive, equitable assessment process, yet it must be implemented within the bounds of available tools and evidence.
Acknowledge measurement error
Despite their widespread use, IQ scores are not infallible and are subject to measurement error. The standard error of measurement (SEM) inherent in IQ testing necessitates caution in interpreting results, especially when scores approach diagnostic thresholds (Flanagan et al., 2022). The conventional cut-off score of 70, often used to demarcate ID, has been criticized for its arbitrary nature and limited predictive validity in clinical practice (Greenspan et al., 2015). Strict adherence to such thresholds disregards the considerable variability in cognitive abilities within individuals with ID, leading to both false positives (identifying individuals as having ID when they do not) and false negatives (failing to identify individuals with ID whose IQ scores exceed 70; Schalock et al., 2021).
Clinicians must therefore consider the SEM and avoid rigid interpretation of numerical cut-offs (Flanagan et al., 2022). A more flexible, criterion-based approach should be used, particularly for borderline scores. Diagnostic decisions should incorporate the full range of criteria, including adaptive behavior, social functioning, and cultural factors. Recognizing the limitations of standardized testing improves diagnostic accuracy and reduces the risk of misclassification. However, it is important to note that in many research contexts, participant classification continues to rely on fixed standard deviation cut-offs (e.g., IQ < 70), rather than incorporating the SEM. This discrepancy between clinical best practices and empirical study design may lead to misclassification and limit the generalizability of research findings. We believe greater alignment is needed between diagnostic guidelines used in clinical practice, such as those outlined in ICD-11 (WHO, 2019), and the inclusion criteria commonly employed in research settings.
Assessment planning and professional collaboration
Employ structural tools
The assessment process should include diagnostic tools that measure both global cognitive functioning and specific cognitive domains. Such tools enable clinicians to identify distinct cognitive strengths and weaknesses and to develop personalized intervention strategies (Luckasson & Schalock, 2015; Schalock et al., 2021). Structural tools grounded in CHC theory provide detailed and nuanced insight into cognitive abilities. While cognitive assessments targeting Stratum II domains typically focus on general intelligence, diagnostic procedures should also include instruments measuring Stratum I and other specific abilities. By identifying relative strengths and weaknesses, clinicians can design interventions that both address specific deficits and leverage existing capabilities to enhance adaptive functioning. Employing these structured tools helps ensure that interventions are aligned with the individual’s cognitive profile, developmental expectations and real-world challenges.
In-depth diagnosis
The process of diagnosing ID should not conclude with a single diagnostic assessment. Given the complexity and multidimensional nature of intellectual functioning, particularly in individuals with MID, it is critical to conduct ongoing, in-depth diagnostic evaluations even after an initial diagnosis has been established (Greenspan et al., 2015). In-depth diagnosis comprises both an initial evaluation and subsequent assessments that consider the dynamic nature of cognitive and adaptive functioning over time. Intellectual disability, especially in the mild range, may present differently at different life stages, with individuals demonstrating fluctuations in adaptive functioning and cognitive development (WHO, 2019; Schalock et al., 2021). Continual assessments also help identify comorbid conditions or other influencing factors, such as mental health disorders, physical health issues, or environmental variables – including family dynamics or educational contexts – that may impact cognitive and adaptive behavior (Burd et al., 2019).
Ongoing assessment allows clinicians to monitor progress, adjust intervention plans, and ensure the provision of appropriate support at each developmental stage. Moreover, in-depth diagnosis captures areas that may not be adequately assessed through standardized tools, including social communication skills and executive functioning deficits. These aspects are crucial for comprehensive understanding of the individual's cognitive profile and should be explored through interviews, observations, and behavioral assessments, particularly when the person’s IQ score is near the diagnostic threshold for ID.
Multidisciplinary teams
One of the most effective strategies for delivering comprehensive care to individuals with ID is engaging multidisciplinary teams. Because ID affects multiple domains – cognitive, social, emotional, and adaptive – a collaborative approach involving various professionals ensures that all facets of the individual's functioning are addressed (Burd et al., 2019; Schalock et al., 2021). Such teams typically include psychologists, special education teachers, speech and language pathologists, occupational therapists, social workers, and medical professionals (Burd et al., 2019). Each team member contributes specialized expertise that facilitates a fuller understanding of the individual’s needs and abilities. Interprofessional collaboration enables the development of a comprehensive, coordinated intervention plan tailored to the individual’s profile across diverse settings. The consistency afforded by this approach enhances intervention outcomes and aligns strategies with the person’s environment and goals (Tassé et al., 2012). Moreover, multidisciplinary teams can support equipping caregivers and family members with the necessary resources and guidance. As families are central to implementing interventions and promoting the well-being of individuals with ID (Blacher et al., 2005; Knox, 2000; Lima-Rodríguez et al., 2018), empowering them ensures continuity of care and improves quality of life.
Understanding heterogeneity
Recognize cognitive profiles
Recent research underscores the importance of identifying distinct cognitive profiles among individuals with ID, rather than treating them as a homogeneous group (Bergeron & Floyd, 2013; Sajewicz-Radtke et al., 2022, 2025b). Large-scale cluster analyses have demonstrated significant intra-group variability among individuals with MID, particularly in verbal reasoning, working memory, visual–spatial processing, and declarative memory (Sajewicz-Radtke et al., 2022, 2025a, 2025b). These studies have revealed functionally meaningful subgroups, such as those with pronounced language-based deficits, low verbal working memory, or relatively preserved nonverbal skills. Such findings illustrate the multidimensional nature of cognitive functioning in ID and reinforce the need to assess both broad and narrow CHC abilities to enhance diagnostic precision and intervention design. Recognizing diverse cognitive configurations is critical for moving beyond reductive, IQ-based assessments and toward more nuanced, person-centered evaluations. This approach aligns with contemporary models such as CHC theory and ICD-11 (WHO, 2019), which emphasize the diagnostic relevance of detailed cognitive profiling across functional domains (Schalock et al., 2021).
Tailor interventions
In response to the variability in cognitive profiles, cognitive interventions should be systematically tailored to reflect each individual's specific constellation of strengths and limitations. Rather than employing uniform protocols, clinicians are advised to design interventions that leverage preserved abilities – such as semantic or visual memory – and compensate for specific deficits in working memory or episodic recall (Singh, 2016). This individualized approach increases the ecological validity of interventions and enhances their practical significance, particularly in educational and adaptive contexts. By aligning interventions with cognitive profiles, this method supports more meaningful, sustainable outcomes.
Additional considerations
Rule out other conditions
During diagnostic evaluations for ID, it is important to consider differential diagnoses that may mimic or exacerbate cognitive impairments. Sensory deficits (e.g., uncorrected hearing or vision impairments), neurodevelopmental conditions such as speech and language disorders, and co-occurring psychiatric conditions (e.g., ADHD, mood or anxiety disorders) may confound the assessment of intellectual and memory functioning if not adequately identified and controlled (Burd et al., 2019). Clinical observations and informant reports must therefore be triangulated with standardized tools to ensure that observed deficits are not secondary manifestations of these conditions. Moreover, current diagnostic frameworks, including ICD-11 and DSM-5, advocate for a comprehensive, multidimensional assessment strategy that integrates neuropsychological data, clinical judgment, and contextual factors (APA, 2022; WHO, 2019).
Consider environmental factors
Cognitive development and memory functioning in individuals with MID are profoundly influenced by environmental and psychosocial determinants. Empirical evidence consistently highlights low socioeconomic status, limited parental education, and restricted access to quality educational resources as key risk factors for delayed cognitive or academic development (Burchinal et al., 2000; Ozkan et al., 2012). Profiles characterized by underdeveloped verbal reasoning and knowledge acquisition may reflect contextual deprivation rather than intrinsic cognitive limitations (Sajewicz-Radtke et al., 2025a; Yang et al., 2021). Therefore, assessment of cognitive profiles must account for environmental influences, particularly when interpreting deficits in crystallized intelligence (Gc), verbal working memory, or declarative memory tasks (Yang et al., 2021). Moreover, ecological data – including school history, home literacy environment, and caregiver support – should be systematically integrated into the diagnostic process to distinguish neurodevelopmental impairment from experience-dependent underachievement.
Longitudinal assessment
Another critical component of diagnostic integrity is the longitudinal assessment of intellectual functioning. Intellectual disability, particularly mild forms, often manifests in a fluid and dynamic manner over time (Fisher et al., 2016; Mervis et al., 2012). As individuals age, they may develop compensatory strategies, or experience shifts in their adaptive functioning. Therefore, it is important to assess not only current cognitive and adaptive abilities but also how these have evolved throughout the individual’s life. This longitudinal perspective is particularly important when evaluating children and adolescents, as their cognitive and adaptive profiles may change significantly throughout development.
Cultural sensitivity
Although most cognitive profiling research has been conducted in Western contexts, it is essential to examine the cross-cultural validity of observed cognitive profiles in individuals with ID. Cultural norms influence the development and expression of adaptive behavior, language use, and learning strategies, all of which are central to cognitive assessment (Allison & Strydom, 2009). Replicating profiling studies in diverse cultural and linguistic settings is necessary to determine whether clusters identified in one population – such as verbal/nonverbal dissociation or low learning efficiency – are generalizable across populations with different educational systems, values, and exposure to standardized testing (Allison & Strydom, 2009). Clinicians must also exercise caution in interpreting test results from culturally and linguistically diverse individuals and employ culturally responsive tools and procedures. This approach improves diagnostic equity while enhancing the relevance of cognitive data for individualized support planning.
Assumption of appropriate diagnostic tools
Necessity of appropriate tools
Accurate assessment of cognitive functioning in individuals with ID requires diagnostic tools that are psychometrically robust, developmentally appropriate, and culturally sensitive. As emphasized in this manuscript, exclusive reliance on global IQ scores may obscure meaningful intra-individual variability and misrepresent the individual’s functional capacities. Therefore, tools that yield detailed profiles across multiple CHC domains – including verbal and nonverbal fluid reasoning, knowledge, working memory, quantitative reasoning, and visual processing – are essential for identifying cognitive strengths and weaknesses (Flanagan et al., 2022; Sajewicz-Radtke et al., 2022; Sitnik-Warchulska et al., 2019). Instrument selection must be guided by the individual’s developmental stage, linguistic background, and cultural context to avoid diagnostic bias and support valid interpretation. At the same time, test results should never be interpreted in isolation.
A core tenet of contemporary diagnostic practice, aligned with frameworks such as DSM-5 and ICD-11, is the integration of multi-method, multi-informant, and multi-contextual data to formulate a comprehensive cognitive profile (APA, 2022; WHO, 2019). One of the most valuable yet underutilized strategies is systematic observation of the individual in their natural environment, be it the home, school, or peer group settings. Observing how the individual navigates everyday cognitive demands, including following routines, solving practical problems, or adapting to new situations, provides essential insights into functional cognition that formal tests may not capture (Stigen et al., 2023). For young children especially, play-based interactions – particularly those involving symbolic play or peer cooperation – offer an important window into executive functioning, working memory, and social cognition (Pellegrini, 2001). These contexts allow for the dynamic assessment of cognitive potential and adaptability beyond the static metrics of norm-referenced tools (Fabio, 2005). Thus, meaningful diagnostic conclusions can only be reached through a comprehensive, multidimensional approach that triangulates standardized assessment results with ecological observations and informant perspectives. Such an integrative model ensures not only diagnostic accuracy but also the development of interventions aligned with the individual’s real-world functioning and contextual needs.
Conclusions
The assessment of cognitive functioning in individuals with MID poses a complex diagnostic challenge that requires moving beyond the longstanding dominance of global IQ scores as the principal classification criterion. While intelligence testing can provide valuable data, overreliance on fixed numerical cut-offs – particularly the conventional threshold of a standard score near 70 – has led to a reductionist, test-driven understanding of ID that inadequately captures the complexities of real-world functioning (Greenspan & Woods, 2014). This “number fixation,” often perceived as objective and scientific, persists despite significant concerns regarding the validity of test norms and the limited scope of psychometric instruments, which typically fail to reflect an individual’s ability to recognize and manage practical or social risks. As a result, current practices risk overlooking the lived experiences of individuals with ID and the contextual factors that shape their adaptive functioning (Greenspan & Woods, 2014; Singh, 2016).
Contemporary diagnostic frameworks increasingly emphasize the need for an integrative, multidimensional approach that incorporates both quantitative psychometric data and qualitative observations of behavior across ecological contexts. Clinicians are thus encouraged to adopt strategies that are developmentally appropriate, culturally informed, and economically viable, while remaining attuned to individual differences in stamina, motivation, and environmental accessibility. Grounding cognitive assessments in comprehensive theoretical models – such as the CHC theory – enables a more structured and conceptually valid evaluation of cognitive strengths and weaknesses. When combined with contextualized, descriptive data on daily functioning and vulnerability, this approach supports diagnostic conclusions that are both more accurate and more person-centered (Flanagan et al., 2022; Greenspan & Woods, 2014). In this light, the field must continue to shift toward integrative assessment models that prioritize understanding over categorization and clinical insight over statistical convenience.
The present framework offers several novel contributions to the evolving discourse on the diagnosis of MID. First, it operationalizes the CHC theory in a MID-specific context, offering a structured way to interpret psychometric data beyond global IQ scores. Second, it emphasizes the diagnostic value of narrow (Stratum I) cognitive abilities, which are often overlooked in favor of broader composite indices, despite their relevance for functional outcomes. Importantly, this perspective highlights the need to assess a wide range of cognitive processes, including those that fulfill criteria for conceptual adaptive behavior (i.e. reading and writing, procedural memory), thereby bridging the gap between intellectual performance and real-world functioning.
Third, the article introduces an integrative model of diagnostic inference that synthesizes cognitive, behavioral, and contextual data into a unified clinical judgment. Although clinicians have long employed such holistic reasoning in practice, its formal recognition in diagnostic systems is only now emerging – most notably in the ICD-11 classification, which places explicit emphasis on adaptive functioning and contextualization rather than rigid categorical thresholds. This shift underscores the importance of aligning clinical expertise with empirical evidence. While the proposed approach may appear intuitive to experienced practitioners, a review of current research practices reveals that individuals are still too often selected for studies based solely on IQ criteria, which limits the generalizability and ecological validity of findings.
Finally, the framework promotes the systematic inclusion of longitudinal and ecological information – such as learning history, developmental milestones, and environmental demands – in the planning of assessments and interventions. Although IQ is often regarded as a relatively stable construct, studies involving individuals with intellectual disabilities indicate that this assumption should be treated with caution, particularly in populations with mild or non-specific forms of ID (Maulik et al., 2011; Whitaker, 2008). Therefore, longitudinal assessment – understood as the repeated measurement of both intellectual and adaptive functioning over time – is a critical component of diagnostic integrity. It allows clinicians to track developmental change, identify emerging strengths and vulnerabilities, and avoid diagnostic decisions based solely on single-time-point evaluations.
This approach is especially relevant when working with children and adolescents, whose cognitive profiles and adaptive competencies may evolve significantly during key developmental transitions (Fisher et al., 2016; Mervis et al., 2012). Importantly, this longitudinality should not be limited to IQ assessment alone. While traditional diagnostic classifications have not typically emphasized change-sensitive approaches, a genuinely person-centered model requires attention to the dynamic and changing nature of functioning across the lifespan. Recognizing that individuals with ID may experience shifts in their needs, support systems, and daily functioning, repeated evaluation enables practitioners to refine intervention plans and adjust support strategies accordingly. Thus, ongoing assessment is not only a methodological recommendation but also an ethical imperative in delivering individualized, developmentally appropriate care.