BACKGROUND
Surgical treatment of obesity is a procedure with high documented effectiveness (Chang et al., 2014). The diversity of treatment effects has led researchers to seek answers to the question of the psychological characteristics of patients that increase the probability of achieving optimal and sustainable body weight reduction (Oltmanns et al., 2020). Surgical societies such as the American Society for Metabolic and Bariatric Surgery (ASMBS), the International Association for Surgical Metabolism and Nutrition (IASMEN), and the Metabolic and Bariatric Surgery Section of the Society of Polish Surgeons (Budzynski et al., 2016) recommend preoperative psychological assessment in the pre-surgical period. The British Obesity Metabolic Surgery Society (BOOMS) issued in 2019 recommendations regarding psychological practice in the pre- and post-operative period, indicating the vital role of a patient’s individual consultation with a clinical psychologist. However, these recommendations do not provide a detailed psychological management plan (Ogden et al., 2019), as the course of the diagnostic process is the decision of the diagnostician based on the patient’s clinical situation and adaptive capacities. The main aim of psychological interventions applied to patients who are candidates for bariatric surgery is to prepare them for this form of treatment, supervising the weight loss process both in the early and long-term postoperative period (Raman et al., 2020), which requires various psychological interventions aimed at changing the patient’s functioning and strengthening their adaptive capacity, including in the area of emotional regulation mechanisms.
In clinical practice, psychological predictors of postoperative effectiveness are assessed on the basis of a semi-structured interview and observation and with the use of selected diagnostic tools (Marek et al., 2016), and evaluation of the psychological state is monitored before and after surgery. The results of the psychological evaluation of candidates for treatment and the orientation of the applied psychological interventions are presented to the interdisciplinary team that takes charge of the patient’s treatment process.
The identification of mechanisms of impaired self-regulation of eating and the implementation of new remedial strategies are of particular significance in the context of sustained change to treatment-friendly eating habits. Increasing the capacity for self-observation forms the foundation of therapeutic interventions in working with the patient with obesity (Fairburn, 2013; Fairburn et al., 2009). An examination of personality is relevant in evaluating the ability to cooperate in the treatment and to comply with the recommendations of the multidisciplinary team. Findings from studies on the personality of patients who were candidates for bariatric treatment from the very beginning demonstrated high heterogeneity within the group (Müller et al., 2014). There are no conclusive data on personality predispositions supporting the expected results of bariatric treatment. Some studies on personality traits in this group indicate higher values of the factor neuroticism and lower or average values of the factors extraversion and conscientiousness (Brunault et al., 2018; O’Dea & Dibley, 2014; Sekuła et al., 2019; Yeo et al., 2021). Personality traits such as openness to experience and agreeableness have been described as undifferentiated in relation to the population norm (Claes et al., 2013; O’Dea & Dibley, 2014). The results of many studies indicate that patients who are candidates for bariatric treatment are characterized by impulsivity and lower frustration tolerance (Brunault et al., 2018; Claes et al., 2013; Espada et al., 2021; Yeo et al., 2021). In the study by Claes et al. (2013) in the pre-bariatric psychological assessment, two personality subtypes emerged: a resilient/high functioning subtype with a ‘normal’ personality profile and an emotional dysregulated/controlled subtype, characterized by high neuroticism and low extraversion/conscientiousness. Emotional dysregulated/undercontrolled patients showed more concerns about eating/weight/shape, more binge eating driven by emotions and external triggers, more psychological complaints (such as depression and anxiety) and more avoidance and depressive coping reactions than resilient/high functioning patients. Some studies indicated that impulsivity remained at a similar level both before and after bariatric treatment (Georgiadou et al., 2014; Rydén et al., 2004) and was associated with a higher incidence of eating disorders and a risk of lower weight loss and/or obesity recurrence (Meany et al., 2014; White et al., 2010). The analysis of personality traits in both healthy and disturbed patients suggests that the trait pattern defined as the ability to self-regulate is a significant predictor of treatment outcomes in this patient group (Generali & De Panfilis, 2018). It has been repeatedly acknowledged that psychological disorders influence treatment outcomes indirectly (Marek et al., 2016), but no consensus has been reached on the characteristics investigated in the absence of psychopathology. Therefore, researchers have suggested that the present objective in this field should be to identify profiles of personality traits that may negatively affect the outcome of treatment, which is essential in the psychological evaluation for bariatric treatment and allows the identification of a group of patients requiring specialist psychological interventions such as emotional regulation skills training during the period prior to surgical treatment (Claes et al., 2013; Monteleone et al., 2019). Consequently, the aim of the study was to investigate and identify similarities and differences in the severity of personality traits of patients who are candidates for surgical treatment of obesity in the context of developing practical recommendations for psychological interventions in the pre- and post-operative period. Furthermore, the aim of the study of the personality traits of patients with morbid obesity is to draw the attention of the medical community to the need for an individualised approach in the process of preparation of a patient for bariatric surgery and to formulate recommendations for diagnosis and psychological interventions towards patients in the pre- and post-operative period.
PARTICIPANTS AND PROCEDURE
PARTICIPANTS
The study group included patients consecutively consulted psychologically between 2021 and 2022 who were candidates for bariatric surgery at the Centre for the Surgical Treatment of Obesity at the University Hospital in Kraków. Study group inclusion criteria:
BMI ≥ 40 kg/m2 – obesity stage III.
BMI 35-39.9 kg/m2 and ≥ 1 obesity complication, e.g. type II diabetes, hypertension, sleep apnoea.
Primary surgical treatment of obesity.
In the case of mental health disorders, the prerequisite for inclusion in the group was stabilisation of the state of health enabling cooperation with the treatment team to be maintained (patients with an unstable course of mental disorders such as schizophrenia, bipolar affective disorders, or depressive disorders were not included in the study group).
Written consent to participate in the study and to process personal data.
The study group included 101 patients (74 females, 27 males) aged between 22 and 64 (M = 40.46, SD = 9.25). The average BMI was 44.88 (SD = 6.18; min = 35, max = 62). Seventy-eight subjects had stage III obesity and 23 subjects had stage II obesity. The included subjects, after giving written consent to participate in the study, were asked to complete the NEO Personality Inventory-Revised (NEO-PI-R). The choice of the tool was dictated by the feasibility of both scientific objectives due to the methodological value of the test and clinical objectives related to the possibility of evaluating the level of adaptation to the treatment. Each respondent received information about the results of the study during the psychological consultation. The psychometric indicators of the Polish version of the questionnaire indicate that the factor structure corresponds to the methodological and theoretical premises of the Big Five Model. For the main factors, internal consistency indicators are high, from .81 to .86, and for most of their components they range from .51 to .70 (Siuta, 2006).
MEASURES
The NEO Personality Inventory-Revised (NEO-PI-R; Costa & McCrae, 1992), in the Polish adaptation by Siuta (2006, 2009), is a tool based on the theoretical Five-Factor Model (FFM) of personality, taking into account taxonomies of five personality factors: neuroticism, extraversion, openness to experience, agreeableness and conscientiousness. Each factor has 6 components that provide a detailed description of the factor. These traits reflect characteristic adaptations that may be modified as a result of one’s own biography and under the influence of external factors (Costa & McCrae, 2005). The FFM model enables the assessment of the structure of personality traits and to a lesser extent relates to mental disorders. The test examines traits of ‘normal’ personality; however, research indicates that increases or decreases in the parameter values of the traits tested may indicate the presence of psychopathological symptoms and/or personality disorders (Malouff et al., 2005; Saulsman & Page, 2004) and are helpful in the assessment of an individual clinical diagnosis (Jankowski et al., 2009). Given the research verifying the FFM model, its hierarchical organisation of features is subject to critical examination (Strus & Cieciuch, 2014). However, the value, both the theoretical value of the FFM model and the NEO-PI-R tool and its clinical application in research, is emphasised by taking into account not only the main personality factors, but also lower-order traits (components of the main factors) (Strus & Cieciuch, 2014). An additional value of the NEO-PI-R tool is its ability to refer to a normalisation group on a sten scale. Subjects score in the following sten ranges: 1 and 2 – very low; 3 and 4 – low; 5 and 6 – medium (population norm); 7 and 8 – high; 9 and 10 – very high.
STATISTICAL ANALYSIS
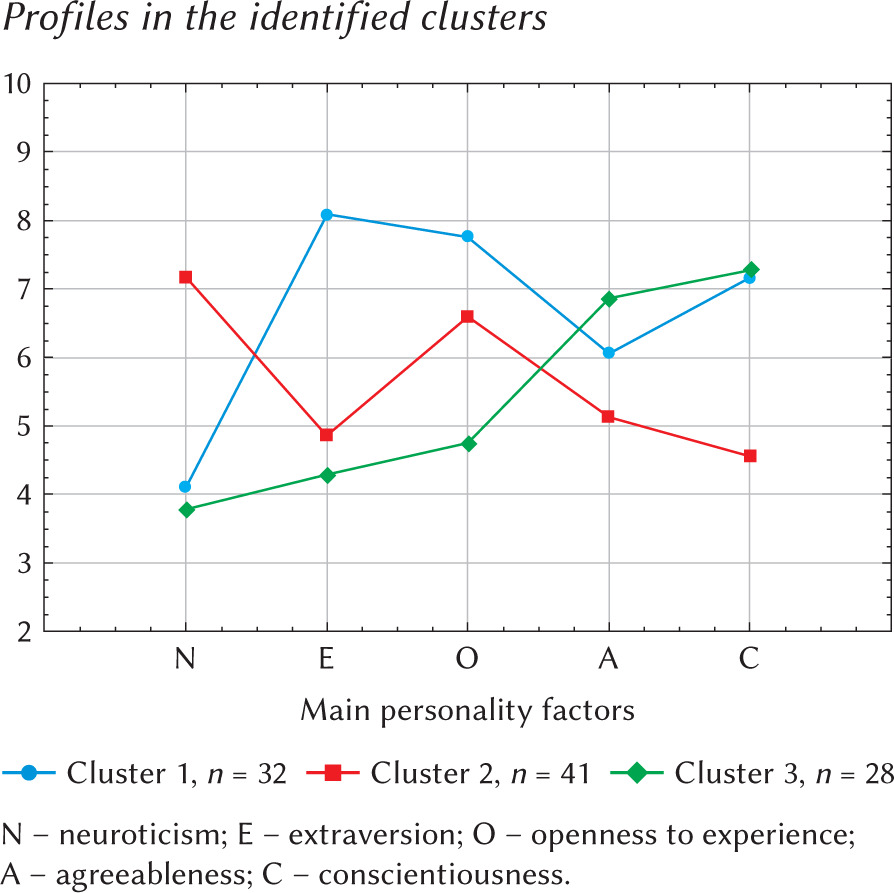
The raw values of the main and component factors of the NEO-PI-R Inventory were converted into gender- and age-sensitive sten values, allowing the values obtained to be compared with population norms. The interpretation adopts the rule that results are rounded to the nearest whole number. The study used the cluster analysis method and three clusters were determined on the basis of agglomeration (Figure 1). A further step was to conduct an analysis of variance using Tukey’s b post-hoc test for differences in personality factors between clusters.
ETHICS STATEMENT
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration of 1975, as revised in 2000. The Bioethics Committee of the Jagiellonian University has approved the study entitled “Psychological predictors of eating behaviour change in bariatric patients – a longitudinal study” (nr of document: 1072.6120.16.2021 of February 17, 2021). Informed consent was obtained from all individual participants included in the study.
RESULTS
A detailed analysis of the main factor subscales illustrates that the value of one component of the neuroticism factor, i.e. N5-impulsiveness (M = 6.77), one component of the conscientiousness factor, i.e. S1-competence (M = 7.08), and the two components of the openness to experience factor, i.e. O5-ideas (M = 6.70) and O6-values (M = 7.45), reach higher values compared to the population norm (Table 1).
Based on the agglomeration, three clusters were determined (Figure 1). The first cluster included 32 people (31.7%), the second cluster included 41 people (40.6%) and the third cluster included 28 people (27.7%).
Analysis of the values in relation to the population norm shows that profile one falls outside the average values in the four main factors. These are high scores for extraversion, openness and conscientiousness and a low score for neuroticism. Profile two is characterised by high scores on the neuroticism and openness to experience scales, with low scores on the conscientiousness scale. The third cluster is characterised by low results in the factor neuroticism and extraversion, and high results in the factors openness to experience, agreeableness and conscientiousness. The means and standard deviations in each cluster for the main personality dimensions in the Big Five model are presented in Table 2, and their graphical representation in sten values is shown in Figure 1.
The analysis indicated different personality characteristics in the clusters. In terms of the main personality factors, cluster 1 and cluster 3 are characterised by low intensity of the factor neuroticism (M = 4.09 and 3.79), in contrast to cluster 2 with a high value of this factor (M = 7.17, p < .001).
Cluster 1 showed statistically significantly higher values for the factor extraversion (M = 8.06, p < .001) in comparison to cluster 2 (M = 4.85, p < .001) and cluster 3, where low values for this factor were recorded (M = 4.29, p < .001).
For the openness to experience factor, the analysis showed that participants in cluster 1 scored higher than both participants in cluster 2 (M = 7.75 vs. M = 6.58, p = .032) and participants in cluster 3 (M = 7.75 vs. M = 4.75, p = .032). The scores of the openness to experience factor in clusters 1 and 2 were higher than the population norm and their values were significantly different from each other.
The highest values in severity of the factor agreeableness were obtained in cluster 3 (M = 6.86, p < .005) in comparison to the severity of this factor in clusters 1 and 2 (M = 6.06 and 5.12). The difference between the results in clusters 2 and 3 was statistically significant (p < .005).
In terms of the last factor, conscientiousness, high scores were recorded in cluster 1 and 3 (M = 7.16, M = 7.29). The results in both clusters were significantly different from those in cluster 2 (M = 4.56, p < .001).
Tables 2 and 3 show the means and standard deviations of the sten values of the main personality factors and the component main factors and the differences between the clusters.
Noteworthy are the components of the factor neuroticism in cluster 2. The values of the N1-anxiety component differ from those in cluster 1 (M = 6.59 vs. M = 4.94, p < .005) and from those in cluster 3 (M = 6.59 vs. M = 4.68, p = .002). The same correlations apply to the N3-depression component, which are higher in cluster 2 in comparison to values in cluster 1 (M = 6.56 vs. M = 4.44, p < .001) and to values in cluster 3 (M = 6.56 vs. M = 4.93, p = .002). The values of the component N4-self-consciousness in cluster 2 are significantly higher in comparison to the values in cluster 1 (M = 6.61 vs. M = 5.00, p = .007). The value of the N5-impulsiveness component in cluster 2 is among the results that are very high in relation to the population norm (sten 9). Individuals in cluster 2 scored high with regard to impulsiveness in comparison to those in cluster 1 (M = 8.56 vs. M = 6.16, p < .001) and in comparison to those in cluster 3 (M = 8.56 vs. M = 4.86, p < .001).
In terms of the factor extraversion, noteworthy are the mean values of the components in cluster 1, which, due to the configuration/profile of the personality traits, was named ‘focus on action’. The values of the E1-kindness component are higher than those in cluster 2 (M = 7.75 vs. M = 5.22, p < .001) and than those in cluster 3 (M = 7.75 vs. M = 6.14, p = .009). In terms of the E2-gregariousness component, the scores of those in cluster 1 were higher in comparison to those in cluster 2 (M = 7.09 vs. M = 5.05, p = .001) and in relation to those in cluster 3 (M = 7.09 vs. M = 4.75, p < .001). The high values of the E3-assertiveness component were significantly different from those obtained in cluster 3 (M = 7.25 vs. M = 5.89, p = .040). Also in terms of the E5-excitement seeking component, significant differences were noted between values in clusters 1 and 3 (M = 6.53 vs. M = 4.86, p = .001). Emotionality in terms of E6-positive emotions differentiated all clusters with the highest values in cluster 1 (M = 7.94 vs. M = 5.90, p < .001) (M = 7.94 vs. M = 5.57, p < .001).
In cluster 1, individuals scored high on all components of the factor openness to experience except the O2 variable. Data analysis in this cluster indicates higher values for the O1-imagination component in comparison to the results in cluster 3 (M = 7.56 vs. M = 4.82, p < .001). The results of the O3-emotionality and O4-actions components were also significantly different from cluster 3 (for O3: M = 7.56 vs. M = 4.71, p < .001; for O4: M = 7.56 vs. M = 5.57, p = .002). All clusters showed similar values of the O6 component, which were above the population norm, but did not differ within clusters (M = 7.66, M = 7.46, M = 7.18).
Table 1
Average sten values for the main personality factors and for the components in the whole group (N = 101)
In terms of the agreeableness factor, noteworthy are the mean values of the components in cluster 3, which, due to the configuration of the personality traits, was named ‘focus on avoidance’. Subjects from this cluster obtained high scores in most components of the U factor except for components U4 and U6. The results in the components U1-trust in others and U3-altruism represent values above the population norm in clusters 1 and 3, but are not significantly different from each other. Concerning the U2-straightforwardness component, high values were obtained by subjects from cluster 3 and are considerably higher than the results of subjects from cluster 2 (M = 7.14 vs. M = 5.15, p < .001).
In terms of the components of the conscientiousness factor, both cluster 1 and cluster 3 individuals obtained scores above the population norm, but not significantly different from each other – in cluster 1 in terms of S1-competence, S3-dutifulness, S4-achievement striving and S5-self-discipline; in cluster 3 in terms of S1, S3, S5 and S6-deliberation.
DISCUSSION
The results will be discussed in three areas:
Personality traits of the subjects in relation to the sten norms in the normalisation group.
Characteristics of the three profiles emerged by cluster analysis of the main personality traits (including their components) in the context of findings from previous studies on the personality of patients who are candidates for surgical treatment of obesity.
Formulating psychological advice based on the obtained results of the examination of personality traits and rules of good clinical practice aimed at sustaining optimal results of bariatric treatment.
Table 2
Means and standard deviations of the sten values of the main personality factors and differences between clusters
Table 3
Means and standard deviations of the component personality factors in each cluster and differences between the components of the main personality factors in the clusters
Personality traits of the subjects in relation to the sten norms in the normalisation group. The present research has an innovative character due to profiling of personality traits based on consistent theoretical (Big Five Model) and methodological premises (NEO-PI-R Inventory), which allows for a more detailed, clinical assessment of personality traits and their profiling, in contrast to research results that include both symptoms of psychopathology and personality traits as well as other cognitive psychological constructs derived from different theoretical hypotheses. Studies of personality traits of bariatric patients mainly use tools to assess basic personality dimensions, such as: the Big-Five Mini-Marker of Personality (Stapleton et al., 2020), an abbreviated version of the NEO-PI-R, which is the NEO-FFI (Fuji et al., 2023), or tools with much lower psychometric properties, e.g. the Myers-Briggs Type Indicator (MBTI; de Figueiredo et al., 2021). A significant number of studies published to date have attempted to differentiate traits in patients using tools that examine psychopathological symptoms as well as symptoms of personality disorders (Bętkowska-Korpała et al., 2021; Marek et al., 2021; Riegel et al., 2022). The NEO-PI-R Inventory used in our research allows for a more detailed, clinical assessment of personality traits and their profiling, which is particularly justified in the context of the heterogeneity of the study group (Müller et al., 2014) and also in the context of clinical studies of somatic patients. In our study group, it is observed that the values for the main personality traits are within the population norm. The results of the available studies are varied. Some indicate higher values for the factor neuroticism and lower or average values for the factors extraversion and conscientiousness (Brunault et al., 2018; O’Dea & Dibley, 2014; Sekuła et al., 2019; Yeo et al., 2021), and the values of the main factors openness to experience and agreeableness, similarly to our study, are described as not different from the population norm (Claes et al., 2013; O’Dea & Dibley, 2014). These differences are probably caused by different survey methodologies and the use of shortened screening methods for examining personality traits. Our study showed that the values of several components of the neuroticism, openness to experience and conscientiousness traits were above the mean sten values, and these are: N5-impulsiveness, O5-ideas, O6-values and S1-competence. This implies that people who are candidates for bariatric treatment are characterised by difficulty in the control of impulses and lower tolerance of frustration. The result is consistent with findings reported by many researchers (Brunault et al., 2018; Claes et al., 2013; Espada et al., 2021; Yeo et al., 2021). The study of Claes et al. (2013) showed that although neuroticism and/or its axial symptom-anxiety decreased at least temporarily in patients after bariatric surgery (Maddi et al., 2001; Rydén et al., 2004; van Hout et al., 2009), impulsiveness remained at similar levels both before and after treatment (Georgiadou et al., 2014; Rydén et al., 2004) and was associated with a higher prevalence of eating disorders and a risk of lower weight loss and/or obesity recurrence (Meany et al., 2014; White et al., 2010). High results in the other components, i.e. O5-ideas, O6-value and S1-competence, indicate a greater willingness to consider both new ideas and recognised social values and a stronger sense of self-competence. These results indicate a tendency to think and reflect on possible actions and a belief in being able to act, which is a cognitive dimension and not necessarily related to engaging in activity (behavioural dimension). The results may be related to the findings of studies on the differences between patients with morbid obesity who are candidates for bariatric surgery and those who do not seek this form of treatment, indicating that the former are more self-steering and better adapted (Federico et al., 2019). However, our study did not show higher rates of the factor conscientiousness and those of its components which relate to the behavioural dimension in psychological functioning.
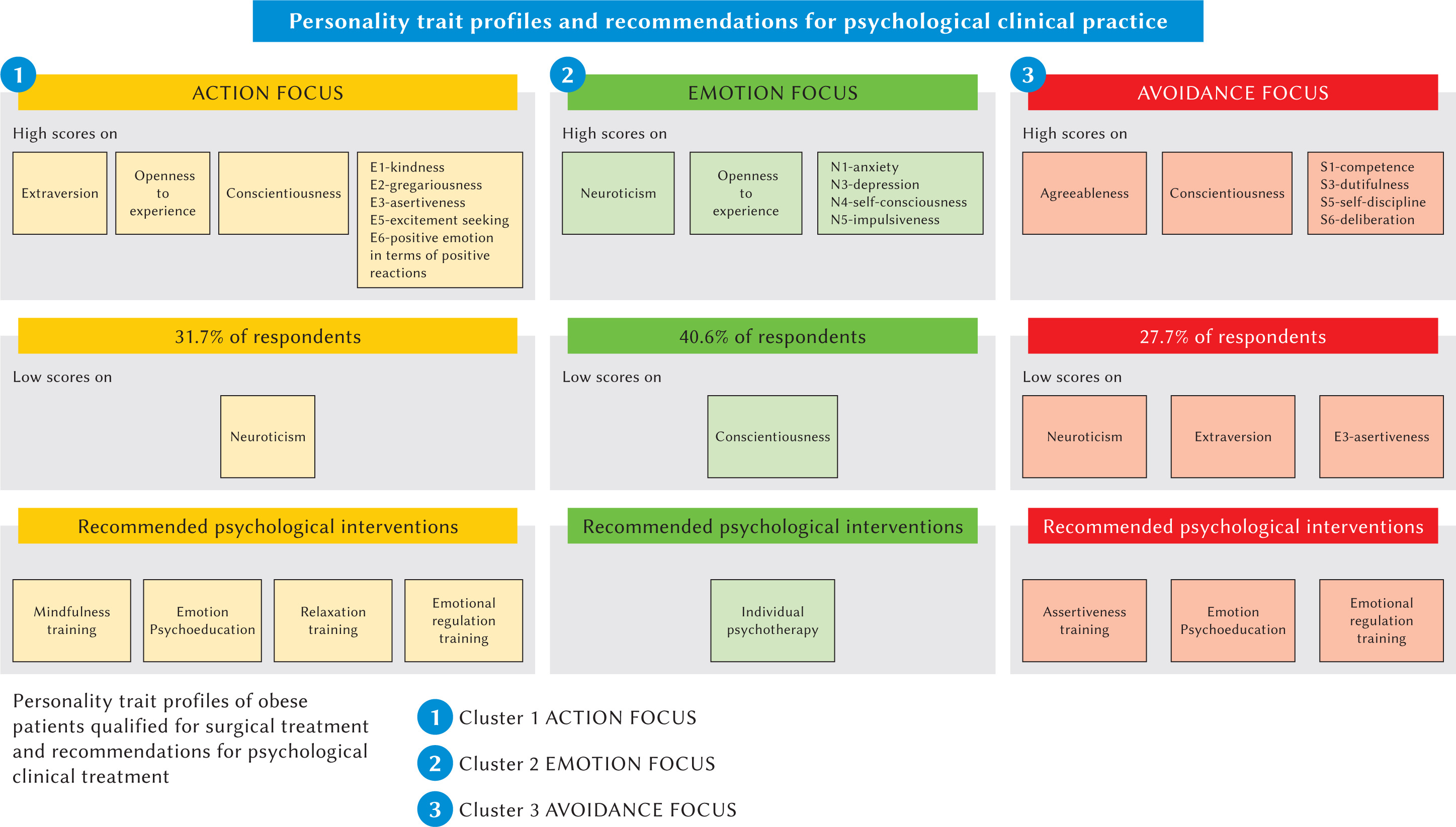
Characteristics of personality trait profiles of obese subjects who are candidates for surgical treatment. Given the characteristic pattern of the main personality traits and their components, the first profile was named ‘action focus’, the second profile was named ‘emotion focus’, and the third profile was named ‘avoidance focus’.
The ‘action-focused’ personality profile is characterised by low scores on the neuroticism factor and high scores on the extraversion, openness to experience and conscientiousness factor in relation to the sten scale (see Table 2). The values of the components of the extraversion factor, i.e. E1-kindness, E2-gregariousness, E3-assertiveness and E6-positive emotion, in terms of positive reactions are significantly higher than both population norms and values in the other clusters (see Table 3). Individuals with this outcome profile are characterised by greater interpersonal comfort and a high need for social stimulation, and consider themselves to have a low vulnerability to stress. They manifest more positive emotions and a cheerful/optimistic attitude, intensely seek sensations and have difficulties in tolerating routine situations. In comparison to those in cluster 3, they clearly differ in terms of the E3-assertiveness component, meaning that they show more ability to take the initiative and dominate in social relationships. Subjects from this cluster are characterised by a greater openness to experience and to consider new ideas and interpretations of experience in relation to the nominative group as well as those from the other clusters. The higher scores obtained for the conscientiousness factor indicate a belief in competence, a readiness to persevere and reliably complete tasks and a high level of aspiration, and in the context of the high U3-altruism values reveal an attitude of concern for others and a readiness to provide help, even at the expense of not achieving one’s own goals. The values of the N2-hostility, anger component show a low level of experiencing anger and frustration also in comparison with individuals from clusters 2 and 3, and the result of the N3-depression component illustrates the low level of experiencing negative emotions such as sadness, guilt or discouragement among individuals from this group in comparison with the normalisation group, as well as in comparison with individuals from the other clusters. These results may favour the tendency to repress negative emotions. Furthermore, the difficulty in identifying them may be manifested by the presence of somatic symptoms arising in response to stress, e.g. the occurrence of increased appetite, exacerbating eating behaviour as a mechanism to regulate psychophysical tension. The strengths of those in focus 1 are a high level of energy and a willingness to persist, which, combined with high interpersonal skills, may encourage cooperation in treatment and maintenance of health-promoting lifestyle changes, e.g. through the introduction of regular physical activity. At the same time, the high demand for social stimulation and the search for intense sensations create a certain risk of over-stimulation, resulting in increased levels of perceived psychophysical tension. These traits, together with the clearly marked low ability to identify negative emotional states in the profile, create a risk of maladaptive eating behaviour to reduce perceived tension and physical discomfort.
The mechanism of emotional regulation through eating behaviour may be observed in subjects within the second profile. The ‘emotion-focused’ personality profile is characterised primarily by a high value of the factor neuroticism and an elevated value of the factor openness (see Table 2). The profile groups people with a marked tendency to experience negative emotional states, i.e. anxiety, concern, guilt, and depression. Individuals with this personality trait profile differ significantly from those in the other two profiles in terms of experiencing anxiety and depression, indicating their difficulties in emotional adjustment. They are excessively self-critical, prone to experiencing feelings of inferiority, shyness and apprehension in social situations. These characteristics differentiate them from those in cluster 1, who are action-oriented. Particularly noteworthy is the very high score obtained in component N5-impulsiveness. The ability to control impulses, needs and temptations is lower compared to subjects in focus 1 and 3, which increases the risk of developing an eating disorder. These results are consistent with previous reports (Meany et al., 2014; Stenbæk et al., 2014; White et al., 2010). For respondents with an ‘emotionally focused’ profile, pursuing tasks persistently to completion despite obstacles and/or setbacks is difficult and often unattainable, which clearly differentiates them from the population as well as the other respondents. This feature may be a major hindrance to the self-implementation of the bariatric team’s complex recommendations, especially as people with this pattern of personality traits will show lower levels of energy, with less need to take action and more willingness to ponder and reflect. A strong feature of the respondents in this group is their high emotional self-awareness. However, the profile illustrates a low capacity for emotional self-regulation, which poses the risk of maladaptive eating behaviour to reduce psychological discomfort, resulting from experienced high levels of negative emotionality such as anxiety, sadness, anger, and guilt.
The ‘avoidance-focused’ personality profile is characterised by low scores on the factors neuroticism and extraversion and high scores on the factors agreeableness and conscientiousness in relation to the sten norms, as well as the other subjects (see Table 2). Particularly worth noting in this personality trait profile are the components of the factors agreeableness and conscientiousness, most of which reached high scores, demonstrating an orientation towards cooperation and effective action. Individuals with this trait profile describe themselves as less vulnerable to stress, as shown by a low score in relation to the population norm for the factor neuroticism and the N6-vulnerability to stress component. Regarding social relations, they are more trusting, straightforward, altruistic and humble compared to the population norm, and characterised by sincerity and concern for the well-being of others compared to those with the ‘emotion-focused’ trait profile. Similarly, those with the trait profile ‘preoccupied with action’ display a higher sense of competence, high dutifulness and self-discipline compared to those in profile 2. However, they show lower levels of activity and energy and their actions are slow, which can make it more difficult to follow recommendations for maintaining regular physical activity on their own. Furthermore, high results on the agreeableness factor indicate a dominant pattern of dependency in social interactions. Individuals with an ‘avoidance-focused’ trait profile are capable of building a therapeutic relationship, which may have a protective value in the context of working diligently towards a long-term treatment outcome. These individuals, like respondents with trait profile type 1, have a low tendency to experience anger and frustration, which may also contribute to reducing the experienced level of psychophysical tension through destructive eating behaviour.
Psychological advice in the treatment of obese patients who are candidates for surgical treatment in the pre- and post-operative period versus personality profiles. A growing number of studies point to the benefits of bariatric patients participating in psychological intervention programmes which provide a protective factor for the sustainability of the obtained treatment results (Cheroutre et al., 2020; David et al., 2020). Given the results of these studies and the knowledge of the heterogeneity of subjects with morbid obesity, it is essential to develop a consistent and reproducible diagnostic and therapeutic regimen in the practice of the clinical psychologist. Data obtained in this study on personality trait profiles clearly demonstrate the need for psychological advice that takes personality trait diagnosis into account.
According to meta-analyses, high intensity of the factor neuroticism and lower intensity of the factor conscientiousness differentiate mental disorder syndromes the most, and also indicate the presence of personality disorders (Malouff et al., 2005; Saulsman & Page, 2004). The personality trait profile of the subjects classified in cluster 2 ‘focus on emotions’ meets these criteria and, with regard to the group of bariatric patients, is similar to the results of the profile analysis by Claes et al. (2013), who identified a dysregulated/uncontrolled emotion subtype characterised by increased neuroticism and low conscientiousness in action. In contrast to our study, this subtype was also characterised by low values in the extraversion dimension. Results from a follow-up study with seven years of observations showed that emotional deregulation, understood as greater intensity and frequency of negative emotions, was associated with lower weight loss and more frequent eating disorders after bariatric surgery (Lavender et al., 2020). Similarly, high levels of impulsiveness as a trait were associated with more frequent occurrence of eating disorders and a risk of lower weight loss and/or obesity relapse (Meany et al., 2014; White et al., 2010). Another study of the personality of patients who received bariatric treatment between 5 and 10 years previously showed that lower BMI values were correlated with high values of the factor conscientiousness (Caltabiano, 2022). The above data illustrate the need for psychometric psychological tools to identify those personality traits that may adversely affect the outcome of surgical treatment and the implementation of therapeutic interventions in the pre-operative period (Espada et al., 2021). The aim may be achieved by supplementing the psychological interview with a personality test with the NEO-PI-R Inventory. As a result of conducting a psychological diagnosis in this manner, more objective data are obtained on the basis of which patients can be referred for specialist therapeutic programmes.
Therefore, it is reasonable to assume that, within the framework of good clinical practice, high values of the neuroticism factor and low values of the conscientiousness factor are indications for referring a patient for participation in a psychotherapeutic programme aimed at improving emotional self-regulation. In our study, this applies to patients with the personality trait profile ‘emotion-focused’. If the values of the factor neuroticism are within the standard range, but its component of impulsivity as an isolated measure is high in the patient’s profile, then monitoring of psychological functioning should also be considered, both before and after bariatric surgery, as interventions to help achieve optimal treatment results and prevent obesity relapse, particularly in light of data on the relatively constant level of this trait in surgically treated patients who did not receive psychological therapy (Georgiadou et al., 2014; Rydén et al., 2004).
In the literature, personality traits such as persistence in pursuing a goal despite the obstacles encountered, a moderate need for novelty and a cooperative rather than competitive attitude have been identified in individuals with a better outcome from bariatric treatment, expressed in terms of greater weight reduction (Generali & De Panfilis, 2018). At the stage of psychological diagnosis, identifying these personality traits and reinforcing them in the relation with the patient encourages the building of a therapeutic alliance, which may become particularly important in the treatment of patients who are characterised by high levels of agreeableness, thus showing dependent personality traits. With regard to the results of our study, patients with a ‘focus on avoidance’ trait profile are predisposed to psychological interventions aimed at improving the identification of emotional states, their understanding and their impact on eating behaviour. Furthermore, in this group, assertiveness training to improve communication of needs, expectations and emotions is justified. Data from our study indicate that this group has difficulties with assertive refusal (avoidance focus profile), which may lead to ignoring one’s own needs, including health. It appears that assertiveness training combined with working on changing negative beliefs about oneself will improve the ability to maintain a healthy lifestyle and the need to have external motivation to initiate health-promoting behaviours will significantly decrease in favour of self-control and self-awareness.
Regarding patients with a personality trait profile named ‘action-focused’, it is noteworthy that high values of the factor extraversion are consistent with findings among obese compared to normal-weight individuals (Armon et al., 2013). Excitement seeking and a high demand for stimulation seem to be of particular importance. Garcia-Ruiz-de-Gordejuela et al. (2017) found that a high demand for novel stimuli was associated with lower weight loss results after bariatric surgery. However, in contrast to their results, in our study the factor extraversion co-occurred with a high value of the factor conscientiousness, which are protective factors for treatment effects (Caltabiano, 2022).
Patients with this personality trait profile similarly to those with an ‘avoidance-focused’ trait profile are predisposed to psychological interventions aimed at improving the identification of emotional states, their understanding and their impact on eating behaviour. Unlike Profile 3, however, they do not require assertiveness training work. Interventions aimed at improving the ability to maintain a balance between arousal and inhibition levels are justified. Increasing awareness and the ability to recognise body signals through mindfulness training and mindfulness techniques seem to be crucial for this group of respondents.
LIMITATIONS
The limitation in this project relates to it being a study conducted at a single centre, which is, however, a reference facility preparing recommendations for the surgical treatment of people with obesity as part of the nationwide KOS-BAR programme. A second limitation is that it is not representative of the entire population of people undergoing surgical treatment for obesity. In this publication, the analyses did not include the association of personality trait profiles with other clinical variables, e.g. eating behaviour disorders and long-term effects of bariatric treatment. This article is the first report of a longitudinal study, and further analyses taking into account a wide range of medical, psychological and sociogeographical variables are planned. The personality trait profiles identified in the study will be analysed in terms of the results obtained from bariatric treatment.
CONCLUSIONS
The results confirm the heterogeneity in terms of personality traits of people with stage II and III obesity entering bariatric treatment.
In a study of the personality of people who are candidates for surgical treatment of obesity, three significantly different personality trait profiles were identified.
2a. The first profile, ‘action-focused’, is characterised by low neuroticism and high openness to experience and conscientiousness as well as extrovertedness, especially in terms of experiencing positive emotionality and sensation seeking related to interpersonal relationships.
2b. The second profile, ‘emotionally focused’, is characterised by low levels of conscientiousness in action and high levels of neuroticism associated with experiencing unpleasant emotional states, as well as a tendency towards impulsive behaviour.
2c. The third profile, ‘avoidance focus’, is characterised by low levels of neuroticism and extraversion and high levels of agreeableness in interpersonal relationships and conscientiousness in action.
Advices for psychological clinical practice:
The results confirm the need for an individualised approach when preparing a patient with obesity for surgical treatment.
As part of comprehensive patient preparation programmes, it is reasonable to conduct a clinical psychological diagnosis of personality in addition to a mental state assessment, since the outcome of this diagnosis indicates adaptation features that may significantly affect the treatment preparation process.
Directed diagnostic and therapeutic interventions are helpful in preparing the patient for surgery. They also serve to prevent the recurrence of maladaptive eating behaviours, increasing the probability of achieving sustained weight reduction, thereby improving long-term treatment success rates and enhancing the patient’s adaptability.
Diagnosis enables psychological interventions to be oriented or patients to be appropriately referred for specialist psychotherapeutic programmes (see Figure 2).