BACKGROUND
The coronavirus disease 2019 (COVID-19) pandemic, caused by the SARS-CoV-2 virus, was first identified in December 2019 in the city of Wuhan, Hubei province, and subsequently spread to more than 210 countries around the world, representing an emergency for international public health (Fofana et al., 2020; Rossi et al., 2020; Wang et al., 2020). On 20 March 2020, Italy had the highest number of cases (41,035) and deaths (3405) due to COVID-19 in Europe and was the second most affected population globally (Sorbello et al., 2020).
A recent literature review on the psychological impact of epidemics and pandemics that have affected the world in recent years showed that both are associated with anxiety, depression, stress and post-traumatic stress disorder (PTSD) symptoms in surviving people (for a review, see Brooks et al., 2020). In the same way, several studies have found that quarantine measures, as well as the COVID-19 pandemic itself, were associated with similar outcomes (Gan et al., 2022; Pandey et al., 2020; Rossi et al., 2020; Wang et al., 2020). Specifically, a recent systematic review and meta-analysis on the general population reported a prevalence of 29.6% for stress and 31.9% for anxiety due to the COVID-19 pandemic (Salari et al., 2020).
Gender differences in the levels of perceived stress and anxiety symptoms have also been documented for COVID-19, both being higher in women than men (di Fronso et al., 2022; Flesia et al., 2020; Rossi et al., 2020; Szabo et al., 2020).
Although many studies have shown the simultaneous increase of perceived stress and anxiety symptoms during the pandemic period – emphasizing greater vulnerability of women than men – they have only partially examined their possible causal relationship with specific COVID-19 stressful events, as well as whether any other psychological factors could decrease or strengthen these possible associations.
In this regard, research based on the emotion regulation model (Gross, 1998a, b; Gross & John, 2003) has highlighted the prominent interaction between perceived stress and emotion regulation strategies in predicting the subsequent manifestation of anxiety symptoms (Martin & Dahlen, 2005; Zahniser & Conley, 2018), underlining the importance of investigating this relationship also in relation to the COVID-19 pandemic.
In light of the above, the general aim of this study was to better understand the causal relationship between COVID-19 stressful events, perceived stress, emotion regulation strategies and anxiety symptoms in women. Specifically, in this study we were interested to identify COVID-19 stressful events which can directly or indirectly influence anxiety symptoms and whether certain psychological factors (perceived stress and emotion regulation strategies) mediate this relationship, thus increasing or decreasing anxiety symptoms in women.
COVID-19 STRESSFUL EVENTS
Research that aimed to analyze the risks factors of mental health outcomes due to previous pandemics (e.g., severe acute respiratory syndrome – SARS, Middle East respiratory syndrome – MERS) indicates that social distancing and quarantine, being a health-care worker, being unemployed and having financial difficulties were related to poorer mental health outcomes (for a review, see Brooks et al., 2020). All the above-mentioned risk factors have also emerged related to COVID-19 pandemic mental health outcomes (e.g., Maaravi & Heller, 2020; Rossi et al., 2020; Spoorthy et al., 2020; Talevi et al., 2020).
As regards in particular the anxiety symptoms, some studies have shown that they are associated with several COVID-19 stressful events, such as health in general and health status related to COVID-19 of their relatives (Maaravi & Heller, 2020), increased use of preventive measures against COVID-19 (Wong et al., 2020), being under quarantine because they are infected or in close proximity to infected people, interruption of work and having experienced a stressful life event due to COVID-19 (Rossi et al., 2020). On the other hand, perceived stress was found to be associated with having experienced a stressful life event due to COVID-19 and working more than usual due to COVID-19 (Rossi et al., 2020), rising essential goods prices (Mousavi et al., 2020), having a family member or a loved one deceased due to COVID-19 (Mousavi et al., 2020; Rossi et al., 2020), having lower self-discipline and the perceptions of lockdown measures as a limitation of personal freedom (Flesia et al., 2020).
As mentioned above, both for perceived stress and anxiety symptoms the effect of COVID-19 stressful events is more pronounced in women than in men (di Fronso et al., 2022; Flesia et al., 2020; Rossi et al., 2020; Szabo et al., 2020).
Taken together, these results suggest that the unexpected nature of the COVID-19 pandemic, as well as the remarkable impact – including potentially deadly – that it might have on one’s own or loved ones’ health, and the social restrictions that it implies, makes it a set of factors able to increase both the levels of perceived stress and anxiety symptoms more in women than men. However, these studies did not investigate in women the effects on perceived stress and anxiety symptoms of other potential stressful events more directly related to COVID-19, such as having contracted the flu during the pandemic period and got tested for COVID-19.
PERCEIVED STRESS
Stress is a set of physiological, cognitive, emotional, or behavioral responses produced following exposure to a physical, social or psychological stimulus – named stressor or stressful events – that actually or apparently threatened the homeostasis, with the goal to re-stablish homeostasis (Chrousos, 2009; Flesia et al., 2020). Depending on the type, timing, and severity of exposure to a stressor, the stress response could be acute or severe/chronic with short- and long-term consequences for physical and psychological health, respectively (Musazzi et al., 2017). Similarly, a distinction is made between acute and chronic stressors (Eckenrode, 1984).
When faced with chronic or severe stress, the overproduction of cortisol compromises the immune response (Morey et al., 2015), thus increasing the risk of contracting an infection and, potentially, complicating the prevention and control of an epidemic (Xu et al., 2020). In addition, chronic stress can have serious consequences for the brain and other organs and lead to the development of physical and neuropsychiatric illness, such as cardiovascular disease (Esler, 2017; Osborne et al., 2020) and anxiety disorders (Chrousos, 2009; Daviu et al., 2019).
As regards the relationship between perceived stress and anxiety symptoms after a stressful event, individuals will make a judgment on the severity of the crisis in terms of perception and cognition, so that there will be a certain degree of physiological and psychological reactions. The anxiety reaction is one of them (Jones-Bitton et al., 2020; Xu et al., 2020).
Inasmuch as individuals can adopt different coping and emotion regulation strategies in the face of stress, their emotional responses to stress can be very heterogeneous (Krishnan & Nestler, 2008; Mennin & Farach, 2007). The literature suggests that a failure in the management of these emotional responses can lead to anxiety disorders (Mennin & Farach, 2007). In the light of this evidence, a growing body of current research considers emotion dysregulation as a shared mechanism that underlies the development, maintenance, and treatment of many stress-related anxiety disorders (Berking & Wupperman, 2012; Renna et al., 2020; Sakiris & Berle, 2019), emphasizing the importance of emotion regulation in adjustment to stress (Hallion et al., 2018).
EMOTION REGULATION STRATEGIES
Emotion regulation (ER) can be defined as the process by which “we influence which emotions we have, when we have them, and how we experience and express them” (Gross, 2002, p. 282). To regulate our emotions we can use a wide variety of strategies. In particular, Gross (1998a) made a distinction between antecedent-focused and response-focused strategies. While the first are used early in the emotion-generation process – namely before appraisals produce a full-blown emotional response – the second are typically applied after the emotion has already been generated (Dryman & Heimberg, 2018; Hu et al., 2014). Among these, the most widely strategies used by individuals, as well as analyzed and characterized in several studies, are cognitive reappraisal (CR) and expressive suppression (ES) (Hu et al., 2014; Rice et al., 2018; Westerlund et al., 2020).
Cognitive reappraisal is an antecedent-focused strategy that consists in the attempt to modify the emotional impact of an emotional-generating situation through its reinterpretation (Dryman & Heimberg, 2018; Hu et al., 2014). It has been shown that the use of cognitive reappraisal to manage positive emotions, such as happiness, increases the felt intensity and the outward expression of these emotions. Conversely, the use of cognitive reappraisal to manage negative emotions, such as anxiety, decreases their felt intensity and outward expression (Andreotti et al., 2013; Gross & John, 2003; Kalokerinos et al., 2015; Nowlan et al., 2016).
Expressive suppression is a response-focused strategy that consists in the inhibition of external expression of emotions, such as “putting on a smile” when one is in a state of anxiety or having a “poker face” when pleased (Dryman & Heimberg, 2018; Gross, 2014; Gross & Thompson, 2007; Hu et al., 2014). It has been shown that the use of expressive suppression to manage negative emotions, such anxiety, increases their felt intensity. Conversely, the use of expressive suppression to manage positive emotions, such as happiness, decreases the felt intensity of these emotions (Campbell-Sills et al., 2006; Gross, 2014; Gross & John, 2003; Kalokerinos et al., 2015).
Based on these premises and in line with several studies (for a review, see Hu et al., 2014), it is possible to assume that the use of cognitive reappraisal and expressive suppression to regulate emotions may mediate processes related to individual adjustment (O’Leary et al., 2017). Specifically, Dryman and Heimberg (2018) and O’Leary et al. (2017) showed that maladaptive emotion regulation strategies can be considered the best predictor of depressive and anxiety symptoms.
ANXIETY
In the study of anxiety, a useful distinction is made between state and trait anxiety (Cattell, 1966; Spielberg, 1983). State anxiety refers to the “psychological and physiological transient reactions directly related to adverse situations in a specific moment” (Leal et al., 2017, p. 148). On the other hand, trait anxiety has been conceptualized as a personality trait that predisposes an individual to feel excessive state anxiety regardless of environmental conditions (Gumus et al., 2016; Leal et al., 2017). The psychological features of a state of anxiety include feelings of tension, apprehension, nervousness and worry while, at a physiological level, it involves activation of the autonomic nervous system with the subsequent manifestation of several symptoms, such as increased blood pressure and heart rate, excessive sweating, nausea, vertigo, and tremor (Spielberger & Rickman, 1990). Although anxiety per se is considered a normal reaction or response to a stressful or threatening situation, which to a certain degree promotes the individual’s adaptation to the environment, when it is sustained, it occurs at inappropriate moments and interferes with the activities of daily living, it becomes maladaptive and can lead to the development of anxiety disorders (Belzung & Griebel, 2001; Daviu et al., 2019; Schmidt, 2020; Sylvers et al., 2011).
In the light of this evidence, it is important to better characterize state anxiety resulting from exposure to COVID-19 stressful events in order to implement appropriate intervention strategies in a timely manner.
AIM OF THE STUDY
Based on the theoretical premises outlined, this study aims to better understand the causal relationship between different COVID-19-related stressful events, perceived stress, emotion regulation strategies, and anxiety symptoms in women. Specifically, we assumed that different COVID-19-related stressful events can directly and indirectly – through perceived stress and emotion regulation strategies – positively predict state anxiety in women. Moreover, we assumed that perceived stress can directly and indirectly predict – through emotion regulation strategies – state anxiety. As regards the indirect and causal relationship between perceived stress and emotion regulation strategies based on the emotion regulation model (Gross, 1998a, b; Gross & John, 2003) and previous studies (e.g., Dryman & Heimberg, 2018; O’Leary et al., 2017) we assumed that perceived stress can positively predict increased use of dysfunctional emotion regulation strategies (i.e., expressive suppression) compared to functional emotion regulation strategies (i.e., cognitive reappraisal) and that the use of dysfunctional emotion regulation can increase anxiety symptoms (mediator effect of emotion regulation strategies between perceived stress and anxiety symptoms; Dryman & Heimberg, 2018; O’Leary et al., 2017).
PARTICIPANTS AND PROCEDURE
PARTICIPANTS
Multiple criteria were considered to estimate the sample size needed to test our mediation model. First, through the use of a G*Power test – assuming a small effect size and setting power at .90 – a sample size of 990 people was suggested. Second, considering our object of study (i.e., stress events related to COVID-19) the required sample size was estimated for a prevalence as low as 3.00% (Cannon & Roe, 1982), suggesting a sample size of 1118 women. Finally, to better characterize the impact of the COVID-19 pandemic on mental health we considered the possibility to exclude participants affected by mental disorders before the COVID-19 pandemic. Following these suggestions a total of 1180 women were included in this study. Forty-eight of these were excluded from the sample because they had reported a doctor diagnosis and/or an ongoing treatment for mental disorders (e.g., anxiety disorder, depression disorder, post-traumatic stress disorder, obsessive-compulsive disorder) before the COVID-19 pandemic.
The final sample was composed of 1132 women living in different Italian regions (North 63.30%, Centre 14.20%, South 18.50%, Islands 4.00%) with a mean age of 40.19 years, ranging from 19 to 83 years (SD = 12.87). The majority of participants held a university degree (55.50%) and a high school diploma (39.50%). Regarding employment status, participants reported being a worker (67.50%), unemployed (13.60%), a student (11.50%), retired (4.10%) and a homemaker (3.00%).
MEASURES
COVID-19 stressful events. Stressful events related to COVID-19 were analyzed with five dichotomous questions presented in the biographical form of the protocol submitted (response alternatives: yes/no). The items were as follows: 1) “Have you contracted the flu during the COVID-19 pandemic?”; 2) “Have you been tested for COVID-19?”; 3) “Have you contracted COVID-19?”; 4) “Has anyone in your family contracted COVID-19?”; 5) “Have you been bereaved due to COVID-19?”.
Perceived Stress Scale (PSS-10). Perceived stress was evaluated through the Italian 10-item version of the Perceived Stress Scale (PSS-10; Cohen et al., 1983; Cohen & Williamson, 1988; Mondo et al., 2021). Each item, scored on a 5-point Likert scale ranging from 0 (never) to 4 (very often), investigates stressful experiences and responses to stress that occurred in the month before the detection. The global PSS-10 score ranges from 0 to 40 with higher scores indicating higher levels of perceived stress. In this study the Cronbach’s α was .77.
Spielberger State-Trait Anxiety Inventory (STAI) X1/R. State anxiety was measured using the Spielberger State-Trait Anxiety Inventory (STAI) X1/R form, which consists of 10 items that are rated on a 4-point Likert scale. Higher scores indicate more state anxiety (Sanavio et al., 1997). In this study the Cronbach’s α was .92.
Emotion Regulation Questionnaire (ERQ-10). The Emotion Regulation Questionnaire (ERQ; Gross & John, 2003) is a 10-item self-report measurement scale, which includes two subscales: cognitive reappraisal (6 items) and expressive suppression (4 items). The items are rated on a 7-point Likert scale ranging from strongly disagree to strongly agree. The scores of all items are added together for each subscale; the higher the total score is, the more frequently are the expressive suppression or cognitive reappraisal strategies used. The Italian version of the ERQ-10 demonstrated good internal consistency and a 2-month test-retest reliability of .67 for cognitive reappraisal and .71 for expressive suppression (Balzarotti et al., 2010). In this study the Cronbach’s α was .90 for cognitive reappraisal and .64 for expressive suppression.
PROCEDURE
An online survey composed of demographic items and the measures of the study was developed using the free software Google Forms. The online survey was distributed during the Italian mandatory lockdown – between 18th and 28th April 2020 – across the national territory through social networking sites such as Facebook, WhatsApp, and Instagram. The participants were informed that participation in the study was voluntary, the survey was confidential, and they could withdraw from the survey at any time if they did not want to continue. Additionally, an on-line consent form was obtained from all participants. Approval for this study was obtained from the Ethical Committee of Calabria Region (Catanzaro, Italy) (no. 157/2020).
DATA ANALYSIS
All analyses were conducted in SPSS and LISREL. Following the suggestions of Stage et al. (2004) a preliminary analysis of correlations was carried out to better define the causal model to be tested later with path analysis.
Path analysis is considered an extension of the regression model aimed to test the fit of a correlation matrix with a causal model (Stage et al., 2004). Path analysis provides estimates of the magnitude and significance of hypothesized causal connections among sets of exogenous and endogenous variables.
Specifically, in this study a causal model with path analysis was used to estimate the paths from exogenous variable related to the COVID-19 pandemic (1. Having contracted the flu during the COVID-19 pandemic; 2. Got tested for COVID-19; 3. Having contracted COVID-19; 4. Having a family member infected by COVID-19; 5. Having experienced bereavement due to COVID-19) and endogenous variables such as perceived stress, cognitive reappraisal, expressive suppression and state anxiety.
To evaluate the causal model goodness of fit we used the following indices: the root mean square error of approximation (RMSEA), the comparative fit index (CFI), the non-normed fit index (NNFI), and the standardized root mean square residual (SRMR). Acceptable model fit was defined by the following multiple cut-off values: RMSEA ≤ .06, CFI ≥ .95, NNFI ≥ .95, SRMR ≤ .08. Moreover, we tested the indirect effects using the product of coefficient method and generated asymmetric confidence intervals using PRODCLIN (MacKinnon et al., 2007).
RESULTS
PRELIMINARY ANALYSIS
Correlation analysis (see Table 1) was carried out. The analysis showed that “having contracted the flu during the COVID-19 pandemic”, “having a family member infected by COVID-19” and “having contracted COVID-19” significantly correlates with perceived stress and/or state anxiety. Moreover, the analysis showed that cognitive reappraisal and expressive suppression significantly correlate with perceived stress and state anxiety.
Table 1
Means, standard deviations, frequencies, percentages and correlations
These findings support the major hypotheses under investigation and emphasize the relevance of using path analysis to determine the direct and indirect associations between exogenous and endogenous variables hypothesized. As suggested by Stage et al. (2004) these results allow us to improve the hypothesized causal model excluding from the subsequent analysis some variables related to COVID-19 that were not found to be significantly associated with the endogenous variables considered, namely: “got tested for COVID-19” and “having experienced bereavement due to COVID-19”.
PATH ANALYSIS
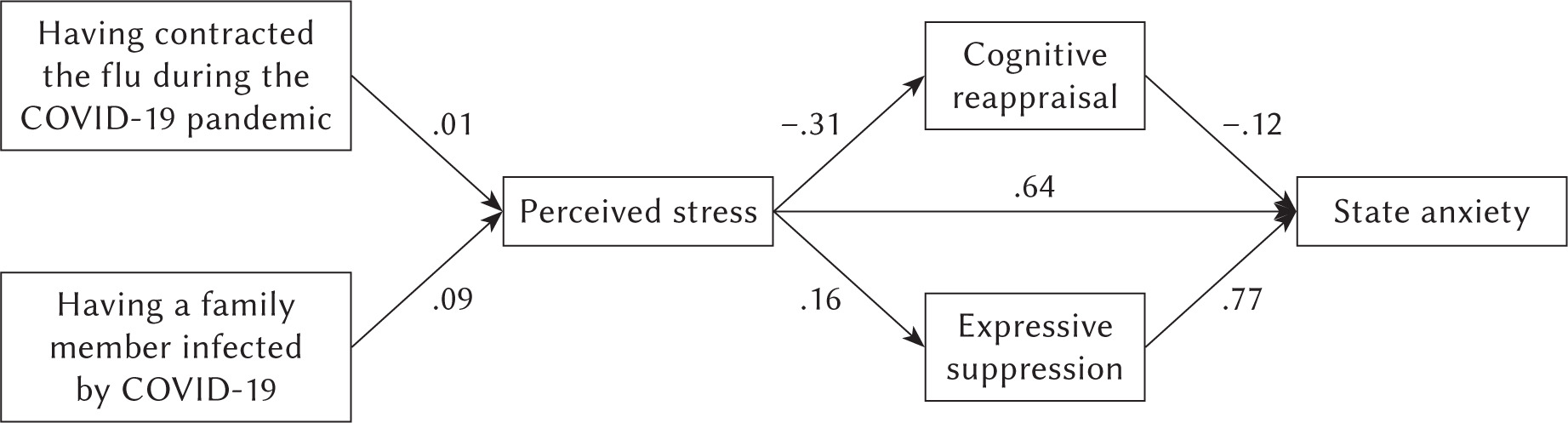
The hypothesized causal model had good fit indices: χ2(5) = 17.70, RMSEA = .037, CFI = .99, NNFI = .097, SRMR = .022. Specifically, as shown in Figure 1, it was found that “having contracted the flu during the COVID-19 pandemic” (SE = .07, t = 2.24) and “having a family member infected by COVID-19” (SE = .09, t = 2.85) were positively related to perceived stress. Moreover, it was found that the relationship between “having contracted COVID-19” and perceived stress (SE = .01, t = 0.44) and state anxiety (SE = –.02, t = 0.97) was not significant. As regards perceived stress, the analysis showed that it was positively related to expressive suppression (SE = .16, t = 5.40) and state anxiety (SE = .64, t = 27.77) and negatively related to cognitive reappraisal (SE = –.31, t = –11.12). Finally, expressive suppression and cognitive reappraisal were, respectively, positively (SE = .77, t = 3.58) and negatively (SE = –.12, t = –4.74) related to state anxiety.
Regarding the significance of the indirect effects, it was found that the 95% confidence intervals for the indirect effect between the “having contracted the flu during the COVID-19 pandemic” and state anxiety ranged from 0.28 to 4.12. The 95% confidence intervals for the indirect effect between “having a family member infected by COVID-19” and state anxiety ranged from 0.56 to 3.11. The 95% confidence intervals for the indirect effect between perceived stress through expressive suppression and state anxiety ranged from 0.01 to 0.02. Finally, the 95% confidence intervals for the indirect effect between perceived stress through cognitive reappraisal and state anxiety ranged from 0.02 to 0.05. All these values did not include a zero, suggesting that all the indirect effects tested are supported. Instead, the 95% confidence intervals for the indirect effect between “having contracted COVID-19” and state anxiety ranged from –2.34 to 3.68, suggesting that this indirect effect tested was not significant.
DISCUSSION
This study aims to better understand the causal relationship between different COVID-19 stressful events, perceived stress, emotion regulation strategies and anxiety symptoms in women. Specifically, in this study we assumed that different COVID-19 stressful events can directly or indirectly influence the state anxiety of women and also that certain psychological factors – perceived stress and emotion regulation strategies – can mediate the relationship between COVID-19 stressful events and state anxiety symptoms. As mentioned above, we decided to focus on women as previous literature shows that, compared to men, the levels of perceived stress and anxiety symptoms are higher in women (McLean & Anderson, 2009; Rincón-Cortés et al., 2019) also in the context of the COVID-19 pandemic (di Fronso et al., 2022; Flesia et al., 2020; Rossi et al., 2020; Szabo et al., 2020).
The analysis carried out confirmed the hypothetical-theoretical model. Regarding the COVID-19 stressful events, we found that only “having contracted the flu during the COVID-19 pandemic” and “having a family member infected by COVID-19” positively predict an increase in the level of perceived stress and indirectly influence the manifestation of state anxiety symptoms in Italian women. Conversely, “got tested for COVID-19”, “having contracted COVID-19” and “having experienced bereavement due to COVID-19” do not predicted an increase in either perceived stress or anxiety symptoms. Our results can be explained by the fact that “having the flu during the COVID-19 pandemic” and “having a family member with COVID-19” are events that may put the individual in a prolonged state of uncertainty with respect to, for example, having a loved one deceased due to COVID-19. This state of uncertainty and doubt about what might happen could lead women to experience more stress and anxiety (Carleton et al., 2012). Moreover, Rossi et al. (2020) showed that having a loved one deceased due to COVID-19 is associated with a lower level of perceived stress and higher post-traumatic stress disorder (PTSD) symptoms but not with anxiety symptoms in an Italian sample, not examining gender differences.
Concerning the fact that the women who reported having tested positive for COVID-19 were able to fill in the questionnaires in a proper manner, we can assume that they were asymptomatic or had mild cases of COVID-19. This could be because “having contracted COVID-19” has no significant effect on perceived stress and anxiety symptoms. Accordingly, Jeong et al. (2020) reported that only asymptomatic or mildly symptomatic patients who had a longer duration of quarantine have experienced anxiety symptoms. In addition, Maaravi and Heller (2020) found that people are more anxious about the health conditions of their relatives than about themselves. Being affected by COVID-19 oneself could lead to perceiving better control of the situation – e.g., by functionally monitoring and evaluating one’s physical symptoms – compared to having a family member with COVID-19, thus limiting the levels of perceived stress and anxiety symptoms. This explanation agrees with the results of AbuRuz et al. (2019) which showed that the perceived control mediates the relationship between anxiety symptoms and postoperative length of stay (LOS) and that the postoperative LOS was higher for female than for male patients.
In line with the emotion regulation model (Gross, 1998a, b; Gross & John, 2003), our results also showed that emotion regulation strategies mediate the relationship between perceived stress and the manifestation of anxiety symptoms (Martin & Dahlen, 2005; Zahniser & Conley, 2018) in women. Specifically, in line with previous studies (e.g., Dryman & Heimberg, 2018; Hu et al., 2014; O’Leary et al., 2017), we found that perceived stress predicts increased use of expressive suppression and decreased use of cognitive reappraisal. In turn, increased use of expressive suppression – compared to cognitive reappraisal – resulted in an increase of anxiety symptoms. Thus, the use of cognitive reappraisal and expressive suppression to regulate emotions mediates the relationship between perceived stress and anxiety symptoms. These results can be partially explained considering that the adoption of different coping and emotion regulation strategies in the face of stress can lead to women experiencing different emotional responses to life events. The ineffective and effective management of these emotional responses, respectively, increases or decreases the manifestation of anxiety symptoms (Mennin & Farach, 2007).
THE THEORETICAL AND PRACTICAL CONTRIBUTION OF THE STUDY
Considering that only a few studies have examined the impact of specific stressful events related to the COVID-19 pandemic on psychological outcomes, we believe that our results have helped to increase our knowledge on this topic. Specifically, the present study shows that COVID-19 stressful events that place women in a state of prolonged future uncertainty (i.e., “having contracted the flu during the COVID-19 pandemic” and “having a family member infected by COVID-19”), can have a greater influence on perceived stress and anxiety symptoms than other stressful events that, although tragic and of impact (e.g., “having experienced bereavement due to COVID-19”), do not generate less uncertainty. Furthermore, in this study, particular emphasis was put on the strategies that can help women to adapt and manage successfully the perceived stress connected to these specific COVID-19 stressful events. As regards the implications for clinical practice, our results make it possible to select the stressful events to which, in the pandemic era, it is necessary to pay particular attention in a clinical setting and suggest the implementation of psychological interventions based on the emotion regulation model (Gross, 1998a, b; Gross & John, 2003) in Italian women. Between these, the third-wave psychological interventions of cognitive behavioral therapy (CBT; Beck, 1976; Klumpp et al., 2017), namely dialectical behavior therapy (DBT; Fassbinder et al., 2016; Linehan, 1993), acceptance commitment therapy (ACT; Hayes et al., 1999; Valdivia-Salas et al., 2010), and mindfulness-based interventions (Chambers et al., 2009; Grecucci et al., 2015), place emotion regulation as an essential direct target of treatment in chronic stress-related pathology such as anxiety and mood disorders (Renna et al., 2020; Sakiris & Berle, 2019).
LIMITATIONS
There are considerable limitations to this research that can be helpful for future studies. First, it is important to recognize that the sampling used is not as effective as true random sampling; nonetheless, it allowed us to overcome specific disadvantages connected with true random sampling such as being overly expensive and time-consuming. Moreover, the participants involved showed heterogeneity in educational qualifications and work experience. In future studies, it may be useful to control the effect of those variables within the model analyzed in this study. As regards the analysis used to test the model, even though a path analysis was performed to examine “causal” hypotheses, the data collected were cross-sectional. In future studies it would be better to use a longitudinal method. Lastly, self-reported measures were administered to assess the dimensions of this study. Future research should take into consideration different methods to reduce the influence of self-report bias.